

Sixteen years of ICPC use in Norwegian primary care: looking through the facts
- PMID: 20181271
- PMCID: PMC2848129
- DOI: 10.1186/1472-6947-10-11
Sixteen years of ICPC use in Norwegian primary care: looking through the facts
Abstract
Background: The International Classification for Primary Care (ICPC) standard aims to facilitate simultaneous and longitudinal comparisons of clinical primary care practice within and across country borders; it is also used for administrative purposes. This study evaluates the use of the original ICPC-1 and the more complete ICPC-2 Norwegian versions in electronic patient records.
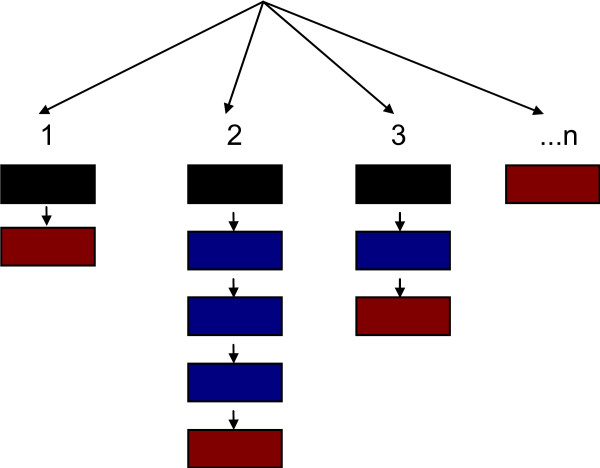
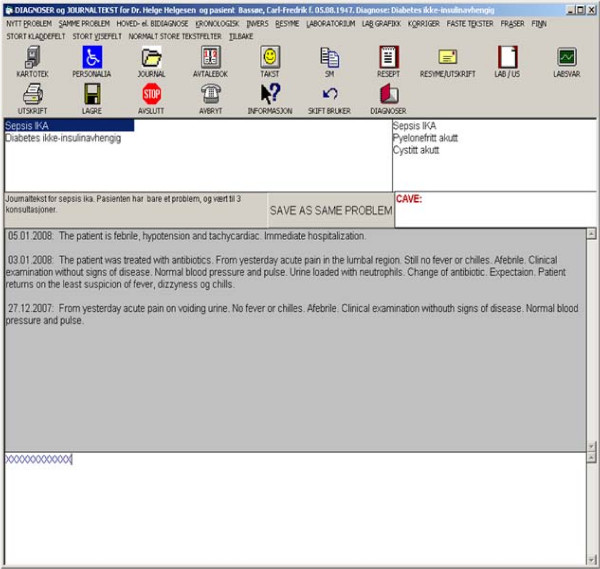
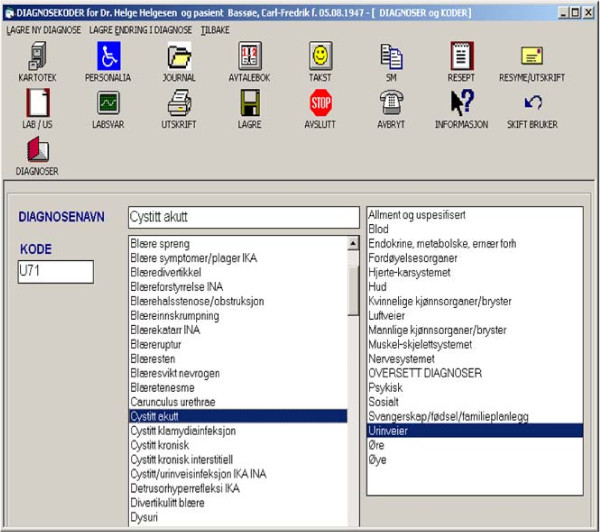
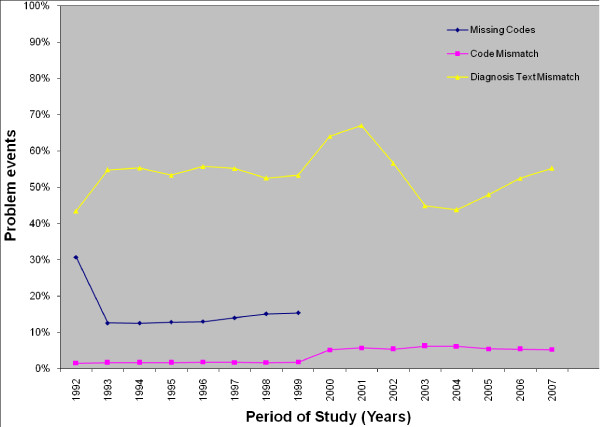
Methods: We performed a retrospective study of approximately 1.5 million ICPC codes and diagnoses that were collected over a 16-year period at 12 primary care sites in Norway. In the first phase of this period (transition phase, 1992-1999) physicians were allowed to not use an ICPC code in their practice while in the second phase (regular phase, 2000-2008) the use of an ICPC code was mandatory. The ICPC codes and diagnoses defined a problem event for each patient in the PROblem-oriented electronic MEDical record (PROMED). The main outcome measure of our analysis was the percentage of problem events in PROMEDs with inappropriate (or missing) ICPC codes and of diagnoses that did not map the latest ICPC-2 classification. Specific problem areas (pneumonia, anaemia, tonsillitis and diabetes) were examined in the same context.
Results: Codes were missing in 6.2% of the problem events; incorrect codes were observed in 4.0% of the problem events and text mismatch between the diagnoses and the expected ICPC-2 diagnoses text in 53.8% of the problem events. Missing codes were observed only during the transition phase while incorrect and inappropriate codes were used all over the 16-year period. The physicians created diagnoses that did not exist in ICPC. These 'new' diagnoses were used with varying frequency; many of them were used only once. Inappropriate ICPC-2 codes were also observed in the selected problem areas and for both phases.
Conclusions: Our results strongly suggest that physicians did not adhere to the ICPC standard due to its incompleteness, i.e. lack of many clinically important diagnoses. This indicates that ICPC is inappropriate for the classification of problem events and the clinical practice in primary care.
Figures
Similar articles
-
ICPC as a standard classification in Norway.Fam Pract. 1996 Aug;13(4):391-6. doi: 10.1093/fampra/13.4.391. Fam Pract. 1996. PMID: 8872099
-
Identifying musculoskeletal conditions in electronic medical records: a prevalence and validation study using the Deliver Primary Healthcare Information (DELPHI) database.BMC Musculoskelet Disord. 2019 May 3;20(1):187. doi: 10.1186/s12891-019-2568-2. BMC Musculoskelet Disord. 2019. PMID: 31053119 Free PMC article.
-
Reliability measurement and ICD-10 validation of ICPC-2 for coding/classification of diagnoses/health problems in an African primary care setting.Fam Pract. 2018 Jul 23;35(4):406-411. doi: 10.1093/fampra/cmx132. Fam Pract. 2018. PMID: 30060181
-
The International Classification of Primary Care (ICPC): new applications in research and computer-based patient records in family practice.Fam Pract. 1996 Jun;13(3):294-302. doi: 10.1093/fampra/13.3.294. Fam Pract. 1996. PMID: 8671139 Review.
-
The coming of age of ICPC: celebrating the 21st birthday of the International Classification of Primary Care.Fam Pract. 2008 Aug;25(4):312-7. doi: 10.1093/fampra/cmn028. Epub 2008 Jun 17. Fam Pract. 2008. PMID: 18562335 Review.
Cited by
-
Association between number of medications and mortality in geriatric inpatients: a Danish nationwide register-based cohort study.Eur Geriatr Med. 2020 Dec;11(6):1063-1071. doi: 10.1007/s41999-020-00390-3. Epub 2020 Sep 9. Eur Geriatr Med. 2020. PMID: 32909235
-
Performance scores in general practice: a comparison between the clinical versus medication-based approach to identify target populations.PLoS One. 2012;7(4):e35721. doi: 10.1371/journal.pone.0035721. Epub 2012 Apr 20. PLoS One. 2012. PMID: 22536430 Free PMC article.
-
Biopsychosocial predictors and trajectories of work participation after transdiagnostic occupational rehabilitation of participants with mental and somatic disorders: a cohort study.BMC Public Health. 2018 Aug 15;18(1):1014. doi: 10.1186/s12889-018-5803-0. BMC Public Health. 2018. PMID: 30111291 Free PMC article. Clinical Trial.
-
Point-of-care testing with CRP in primary care: a registry-based observational study from Norway.BMC Fam Pract. 2015 Nov 19;16:170. doi: 10.1186/s12875-015-0385-8. BMC Fam Pract. 2015. PMID: 26585447 Free PMC article.
-
Methods to identify the target population: implications for prescribing quality indicators.BMC Health Serv Res. 2010 May 26;10:137. doi: 10.1186/1472-6963-10-137. BMC Health Serv Res. 2010. PMID: 20504307 Free PMC article.
References
-
- WONCA. ICPC-2-R: International Classification of Primary Care. Oxford: Oxford University Press; 2005.
-
- de Lusignan S, Wells SE, Hague NJ, Thiru K. Managers see the problems associated with coding clinical data as a technical issue whilst clinicians also see cultural barriers. Methods Inf Med. 2003;42(4):416–422. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
