

The Health and Recovery Peer (HARP) Program: a peer-led intervention to improve medical self-management for persons with serious mental illness
- PMID: 20185272
- PMCID: PMC2856811
- DOI: 10.1016/j.schres.2010.01.026
The Health and Recovery Peer (HARP) Program: a peer-led intervention to improve medical self-management for persons with serious mental illness
Abstract
Objectives: Persons with serious mental illnesses (SMI) have elevated rates of comorbid medical conditions, but may also face challenges in effectively managing those conditions.
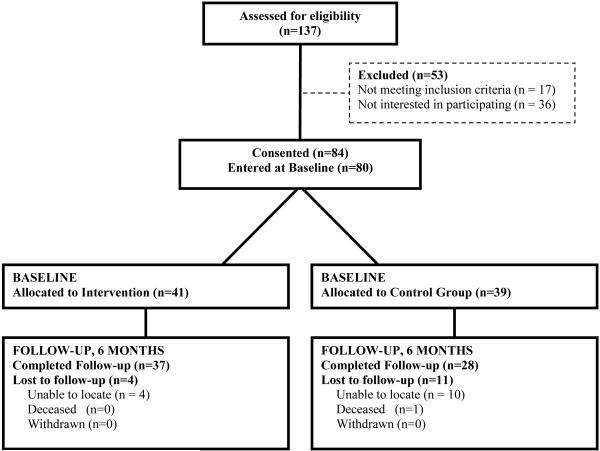
Methods: The study team developed and pilot-tested the Health and Recovery Program (HARP), an adaptation of the Chronic Disease Self-Management Program (CDSMP) for mental health consumers. A manualized, six-session intervention, delivered by mental health peer leaders, helps participants become more effective managers of their chronic illnesses. A pilot trial randomized 80 consumers with one or more chronic medical illness to either the HARP program or usual care.
Results: At six month follow-up, participants in the HARP program had a significantly greater improvement in patient activation than those in usual care (7.7% relative improvement vs. 5.7% decline, p=0.03 for group *time interaction), and in rates of having one or more primary care visit (68.4% vs. 51.9% with one or more visit, p=0.046 for group *time interaction). Intervention advantages were observed for physical health related quality of life (HRQOL), physical activity, medication adherence, and, and though not statistically significant, had similar effect sizes as those seen for the CDSMP in general medical populations. Improvements in HRQOL were largest among medically and socially vulnerable subpopulations.
Conclusions: This peer-led, medical self-management program was feasible and showed promise for improving a range of health outcomes among mental health consumers with chronic medical comorbidities. The HARP intervention may provide a vehicle for the mental health peer workforce to actively engage in efforts to reduce morbidity and mortality among mental health consumers.
Copyright (c) 2010 Elsevier B.V. All rights reserved.
Similar articles
-
Peer-Led Self-Management of General Medical Conditions for Patients With Serious Mental Illnesses: A Randomized Trial.Psychiatr Serv. 2018 May 1;69(5):529-535. doi: 10.1176/appi.ps.201700352. Epub 2018 Feb 1. Psychiatr Serv. 2018. PMID: 29385952 Free PMC article. Clinical Trial.
-
Integrating behavioral healthcare for individuals with serious mental illness: A randomized controlled trial of a peer health navigator intervention.Schizophr Res. 2017 Apr;182:135-141. doi: 10.1016/j.schres.2016.10.031. Epub 2016 Oct 25. Schizophr Res. 2017. PMID: 27793514 Clinical Trial.
-
Home-based, peer-led chronic illness self-management training: findings from a 1-year randomized controlled trial.Ann Fam Med. 2009 Jul-Aug;7(4):319-27. doi: 10.1370/afm.996. Ann Fam Med. 2009. PMID: 19597169 Free PMC article. Clinical Trial.
-
Comparing Two Ways to Help Patients Get Follow-up Care after a Mental Health Visit to the Emergency Room—The EPIC Study [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 May. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 May. PMID: 38484096 Free Books & Documents. Review.
-
Self-management support interventions for persons with chronic disease: an evidence-based analysis.Ont Health Technol Assess Ser. 2013 Sep 1;13(9):1-60. eCollection 2013. Ont Health Technol Assess Ser. 2013. PMID: 24194800 Free PMC article. Review.
Cited by
-
Interventions to Address Medical Conditions and Health-Risk Behaviors Among Persons With Serious Mental Illness: A Comprehensive Review.Schizophr Bull. 2016 Jan;42(1):96-124. doi: 10.1093/schbul/sbv101. Epub 2015 Jul 28. Schizophr Bull. 2016. PMID: 26221050 Free PMC article. Review.
-
Study protocol of a randomized controlled trial evaluating home treatment with peer support for acute mental health crises (HoPe).BMC Psychiatry. 2022 Sep 19;22(1):619. doi: 10.1186/s12888-022-04247-w. BMC Psychiatry. 2022. PMID: 36123649 Free PMC article.
-
Improving Physical Health in Patients With Chronic Mental Disorders: Twelve-Month Results From a Randomized Controlled Collaborative Care Trial.J Clin Psychiatry. 2017 Jan;78(1):129-137. doi: 10.4088/JCP.15m10301. J Clin Psychiatry. 2017. PMID: 27780336 Free PMC article. Clinical Trial.
-
The Wellness Incentive and Navigation intervention improved health-related quality of life among Medicaid enrollees: A randomized pragmatic clinical trial.Health Serv Res. 2019 Dec;54(6):1156-1165. doi: 10.1111/1475-6773.13235. Epub 2019 Oct 22. Health Serv Res. 2019. PMID: 31642066 Free PMC article. Clinical Trial.
-
Clinical Outcomes in Routine Evaluation Measures for Patients Discharged from Acute Psychiatric Care: Four-Arm Peer and Text Messaging Support Controlled Observational Study.Int J Environ Res Public Health. 2022 Mar 23;19(7):3798. doi: 10.3390/ijerph19073798. Int J Environ Res Public Health. 2022. PMID: 35409483 Free PMC article. Clinical Trial.
References
-
- Aday LA. Health status of vulnerable populations. Annu Rev Public Health. 1994;15:487–509. - PubMed
-
- Brown S, Birtwistle J, et al. The unhealthy lifestyle of people with schizophrenia. Psychol Med. 1999;29(3):697–701. - PubMed
-
- Brownson RC, Eyler AA, et al. Reliability of information on physical activity and other chronic disease risk factors among US women aged 40 years or older. Am J Epidemiol. 1999;149(4):379–91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
