

Heterogeneity in the validity of administrative-based estimates of immunization coverage across health districts in Burkina Faso: implications for measurement, monitoring and planning
- PMID: 20185529
- PMCID: PMC3072827
- DOI: 10.1093/heapol/czq007
Heterogeneity in the validity of administrative-based estimates of immunization coverage across health districts in Burkina Faso: implications for measurement, monitoring and planning
Abstract
Background: Data aggregation in national information systems begins at the district level. Decentralization has given districts a lead role in health planning and management, therefore validity of administrative-based estimates at that level is important to improve the performance of immunization information systems.
Objective: To assess the validity of administrative-based immunization estimates and their usability for planning and monitoring activities at district level.
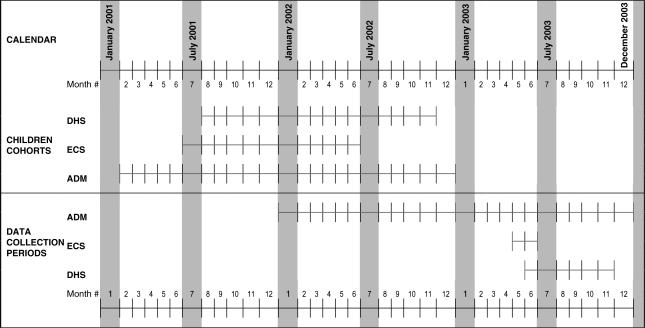
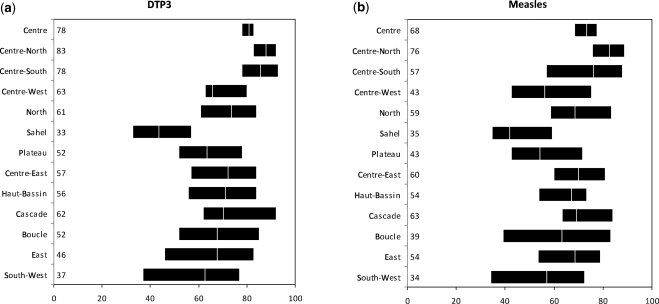
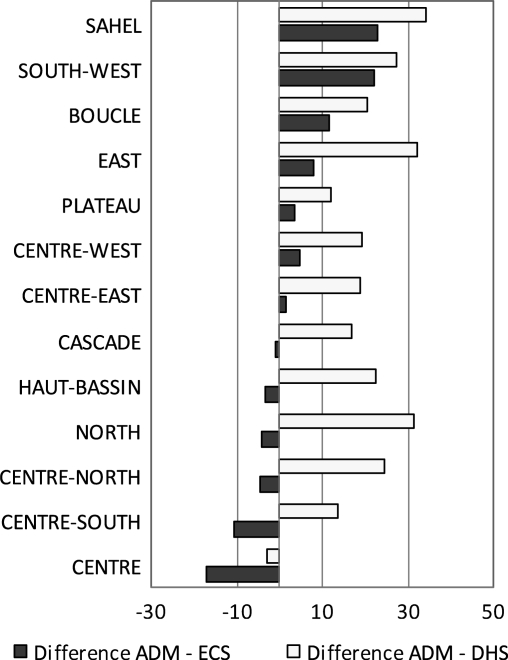
Methods: DTP3 and measles coverage rates from administrative sources were compared with estimates from the EPI cluster survey (ECS) and Demographic and Health Survey (DHS) carried out in 2003 at national and regional levels. ECS estimates were compared with administrative rates across the 52 districts, which were classified into three groups: those where administrative rates were underestimating, overestimating or concordant with ECS estimates (differences within 95% CI of ECS rate).
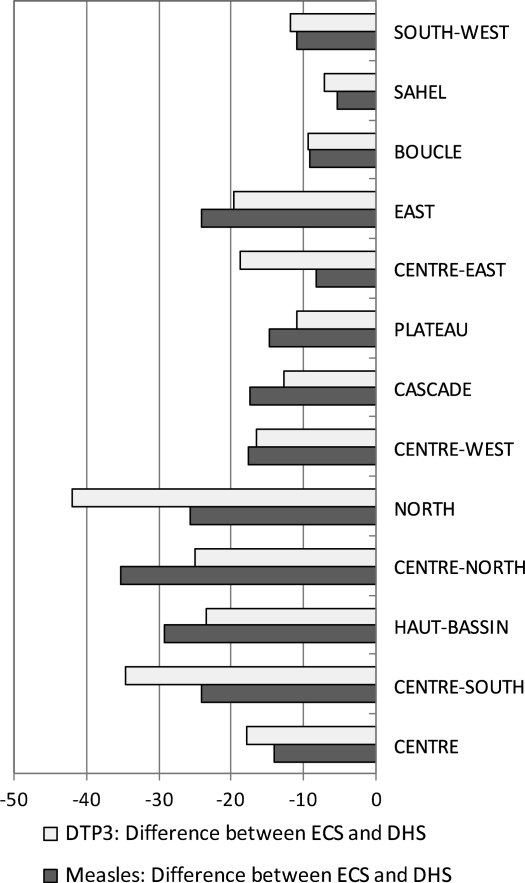
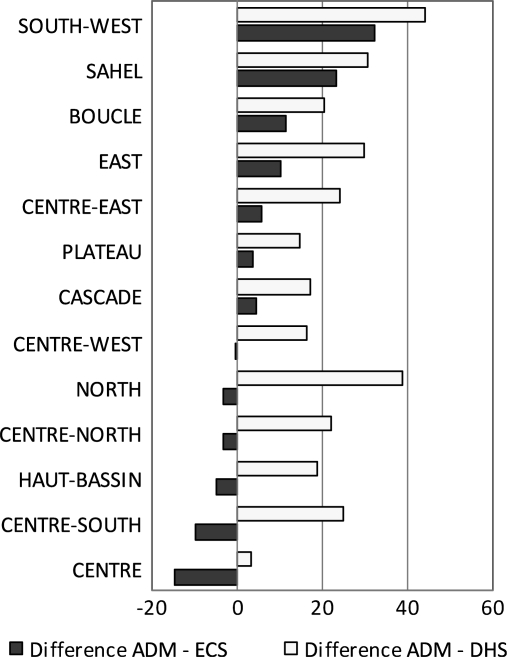
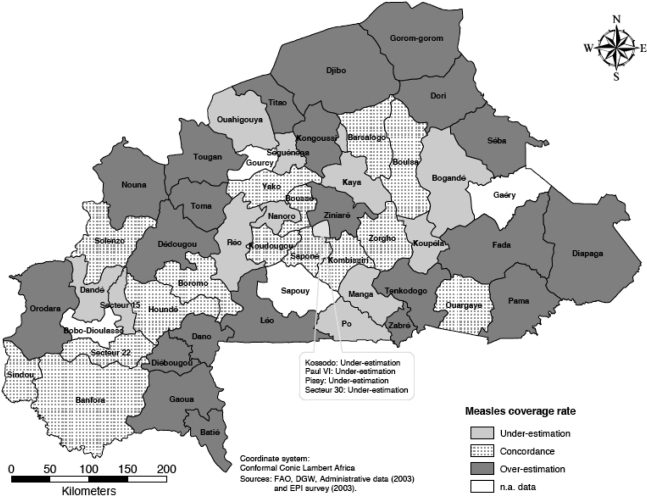
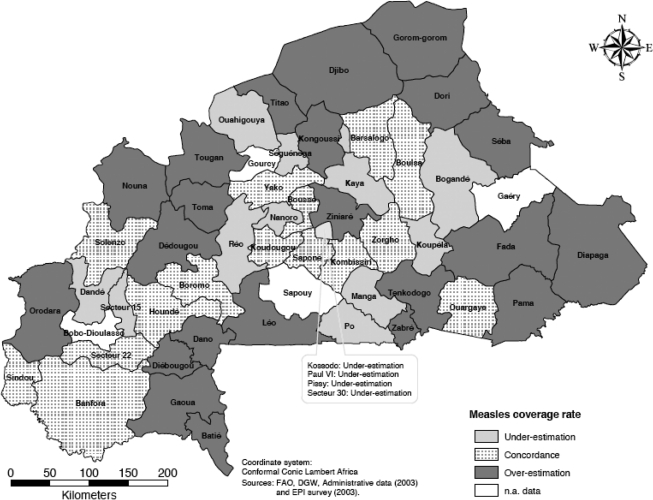
Results: National rates provided by administrative data and ECS are similar (74% and 71% for DTP3 and 68% and 66% for measles, respectively); DHS estimates are much lower. Regional administrative data show large discrepancies when compared against ECS and DHS data (differences sometimes reaching 30 percentage points). At district level, geographical area is correlated with over- or underestimation by administrative sources, which overestimate DTP3 and measles coverage in remote areas. Underestimation is observed in districts near urban and highly populated centres. Over- and underestimation are independent of the antigen under consideration.
Conclusions: Variability in immunization coverage across districts highlights the limitations of using nationally aggregated indicators. If district data are to be used in monitoring and planning immunization programmes as intended by decentralization, heterogeneity in their validity must be reduced. The authors recommend: (1) strengthening administrative data systems; (2) implementing indicators that are insensitive to population mobility; (3) integrating surveys into monitoring processes at the subnational level; (4) actively promoting the use of coverage information by local personnel and district-level staff.
Figures
Similar articles
-
Validity of reported vaccination coverage in 45 countries.Lancet. 2003 Sep 27;362(9389):1022-7. doi: 10.1016/S0140-6736(03)14411-X. Lancet. 2003. PMID: 14522532
-
Use of administrative data to estimate mass vaccination campaign coverage, Burkina Faso, 1999.J Infect Dis. 2003 May 15;187 Suppl 1:S86-90. doi: 10.1086/368052. J Infect Dis. 2003. PMID: 12721897
-
Immunization coverage in young children: a study nested into a health and demographic surveillance system in Burkina Faso.J Trop Pediatr. 2013 Jun;59(3):187-94. doi: 10.1093/tropej/fms075. Epub 2013 Jan 29. J Trop Pediatr. 2013. PMID: 23363884
-
A review of geospatial methods for population estimation and their use in constructing reproductive, maternal, newborn, child and adolescent health service indicators.BMC Health Serv Res. 2021 Sep 13;21(Suppl 1):370. doi: 10.1186/s12913-021-06370-y. BMC Health Serv Res. 2021. PMID: 34511089 Free PMC article. Review.
-
Estimation of infant vaccination coverage at national and region level in Ethiopia: a cross-sectional study.Pan Afr Med J. 2022 Jun 7;42:101. doi: 10.11604/pamj.2022.42.101.18299. eCollection 2022. Pan Afr Med J. 2022. PMID: 36034045 Free PMC article. Review.
Cited by
-
Estimating population-based coverage of reproductive, maternal, newborn, and child health (RMNCH) interventions from health management information systems: a comprehensive review.BMC Health Serv Res. 2021 Oct 25;21(Suppl 2):1083. doi: 10.1186/s12913-021-06995-z. BMC Health Serv Res. 2021. PMID: 34689787 Free PMC article. Review.
-
Assessing strategies for increasing urban routine immunization coverage of childhood vaccines in low and middle-income countries: A systematic review of peer-reviewed literature.Vaccine. 2016 Nov 4;34(46):5495-5503. doi: 10.1016/j.vaccine.2016.09.038. Epub 2016 Sep 28. Vaccine. 2016. PMID: 27692772 Free PMC article.
-
Data management needs assessment for the scale-up of district health information system and introduction of routine (essential) immunization module in Bauchi State, Nigeria, 2015.Pan Afr Med J. 2022 Feb 17;40(Suppl 1):13. doi: 10.11604/pamj.supp.2022.40.1.32458. eCollection 2021. Pan Afr Med J. 2022. PMID: 36157562 Free PMC article.
-
Whom and where are we not vaccinating? Coverage after the introduction of a new conjugate vaccine against group A meningococcus in Niger in 2010.PLoS One. 2012;7(1):e29116. doi: 10.1371/journal.pone.0029116. Epub 2012 Jan 20. PLoS One. 2012. PMID: 22276104 Free PMC article.
-
Coverage, inequity and predictors of hepatitis B birth vaccination in Myanmar from 2011-2016: results from a national survey.BMC Health Serv Res. 2022 Apr 19;22(1):516. doi: 10.1186/s12913-022-07902-w. BMC Health Serv Res. 2022. PMID: 35436953 Free PMC article.
References
-
- Balraj V, Mukundan S, Samuel R, John TJ. Factors affecting immunization coverage levels in a district of India. International Journal of Epidemiology. 1993;22:1146–53. - PubMed
-
- Bishai DM. Global initiatives in universal childhood immunisation. The Lancet. 2008;372:2004–5. - PubMed
-
- Boerma JT, Sommerfelt AE, Rutstein SO, Rojas G. Columbia, MD: Institute for Resource Development; 1990. Immunization: levels, trends and differentials. DHS Comparative Studies No. 1.
