

Phase IIB/III trial of tenecteplase in acute ischemic stroke: results of a prematurely terminated randomized clinical trial
- PMID: 20185783
- PMCID: PMC2860601
- DOI: 10.1161/STROKEAHA.109.572040
Phase IIB/III trial of tenecteplase in acute ischemic stroke: results of a prematurely terminated randomized clinical trial
Abstract
Background and purpose: Intravenous alteplase (rtPA) remains the only approved treatment for acute ischemic stroke, but its use remains limited. In a previous pilot dose-escalation study, intravenous tenecteplase showed promise as a potentially safer alternative. Therefore, a Phase IIB clinical trial was begun to (1) choose a best dose of tenecteplase to carry forward; and (2) to provide evidence for either promise or futility of further testing of tenecteplase versus rtPA. If promise was established, then the trial would continue as a Phase III efficacy trial comparing the selected tenecteplase dose to standard rtPA.
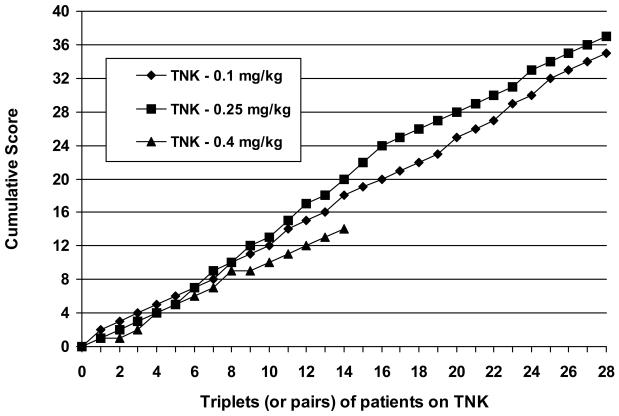
Methods: The trial began as a small, multicenter, randomized, double-blind, controlled clinical trial comparing 0.1, 0.25, and 0.4 mg/kg tenecteplase with standard 0.9 mg/kg rtPA in patients with acute stroke within 3 hours of onset. An adaptive sequential design used an early (24-hour) assessment of major neurological improvement balanced against occurrence of symptomatic intracranial hemorrhage to choose a "best" dose of tenecteplase to carry forward. Once a "best" dose was established, the trial was to continue until at least 100 pairs of the selected tenecteplase dose versus standard rtPA could be compared by 3-month outcome using the modified Rankin Scale in an interim analysis. Decision rules were devised to yield a clear recommendation to either stop for futility or to continue into Phase III.
Results: The trial was prematurely terminated for slow enrollment after only 112 patients had been randomized at 8 clinical centers between 2006 and 2008. The 0.4-mg/kg dose was discarded as inferior after only 73 patients were randomized, but the selection procedure was still unable to distinguish between 0.1 mg/kg and 0.25 mg/kg as a propitious dose at the time the trial was stopped. There were no statistically persuasive differences in 3-month outcomes between the remaining tenecteplase groups and rtPA. Symptomatic intracranial hemorrhage rates were highest in the discarded 0.4-mg/kg tenecteplase group and lowest (0 of 31) in the 0.1-mg/kg tenecteplase group. Neither promise nor futility could be established.
Conclusion: This prematurely terminated trial has demonstrated the potential efficiency of a novel design in selecting a propitious dose for future study of a new thrombolytic agent for acute stroke. Given the truncation of the trial, no convincing conclusions can be made about the promise of future study of tenecteplase in acute stroke.
Trial registration: ClinicalTrials.gov NCT00252239.
Figures
References
-
- Brown DL, Barsan WG, Lisabeth LD, Gallery ME, Morgenstern LB. Survey of emergency physicians about recombinant tissue plasminogen activator for acute ischemic stroke. Ann Emerg Med. 2005;46:56–60. - PubMed
-
- Assessment of the Safety and Efficacy of a New Thrombolytic (ASSENT-2) Investigators Single bolus tenecteplase compared with front-loaded alteplase in acute myocardial infarction: the ASSENT-2 double-blind randomized trial. Lancet. 1999;354:716–722. - PubMed
-
- Haley EC, Lyden PD, Johnston KC, Hemmen TM, the TNK in Stroke Investigators A pilot dose-escalation safety study of tenecteplase in acute ischemic stroke. Stroke. 2005;36:607–612. - PubMed
-
- Brown DL, Johnston KC, Wagner DP, Haley EC. Predicting major neurological improvement with intravenous tissue plasminogen activator treatment of stroke. Stroke. 2004;35:147–150. - PubMed
-
- Lyden P, Raman R, Liu L, Grotta J, Broderick J, Olson S, Shaw S, Spilker J, Meyer B, Emr M, Warren M, Marler J. NIHSS traning and certification using a new digital video disk is reliable. Stroke. 2005;36:2446–2449. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
