

Population-based study of contralateral prophylactic mastectomy and survival outcomes of breast cancer patients
- PMID: 20185801
- PMCID: PMC4415082
- DOI: 10.1093/jnci/djq018
Population-based study of contralateral prophylactic mastectomy and survival outcomes of breast cancer patients
Abstract
Background: Despite increased demand for contralateral prophylactic mastectomy (CPM), the survival benefit of this procedure remains uncertain.
Methods: We used the Surveillance, Epidemiology, and End Results database to identify 107 106 women with breast cancer who had undergone mastectomy for treatment between 1998 and 2003 and a subset of 8902 women who also underwent CPM during the same period. Associations between predictor variables and the likelihood of undergoing CPM were evaluated by use of chi(2) analyses. Risk-stratified (estrogen receptor [ER] status, stage, and age) adjusted survival analyses were performed by using Cox regression. Statistical tests were two-sided.
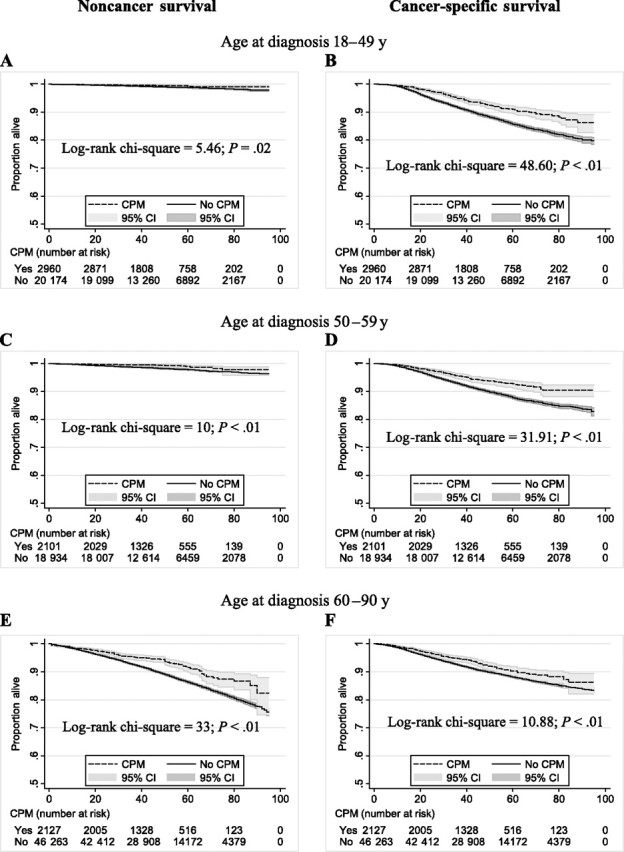
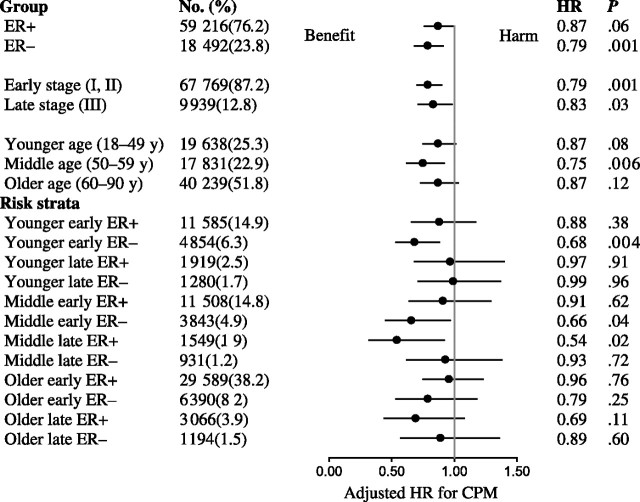
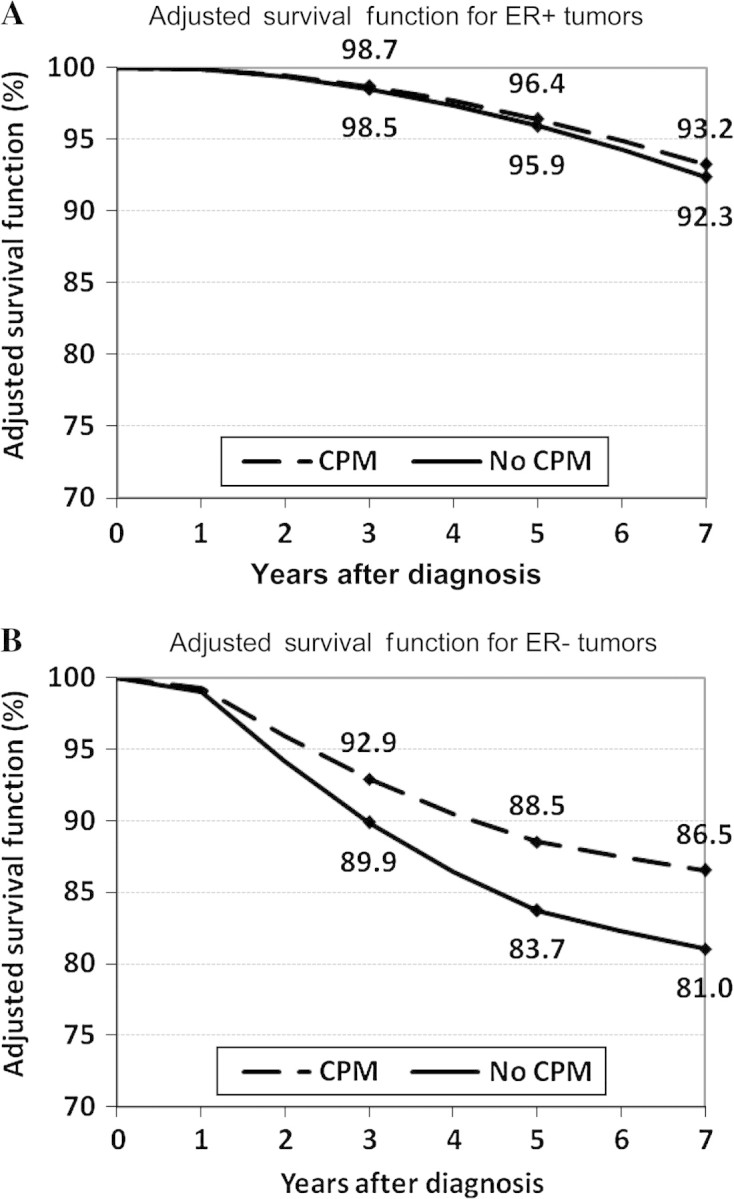
Results: In a univariate analysis, CPM was associated with improved disease-specific survival (hazard ratio [HR] of death = 0.63, 95% confidence interval [CI] = 0.57 to 0.69; P < .001). Risk-stratified analysis showed that this association was because of a reduction in breast cancer-specific mortality in women aged 18-49 years with stages I-II ER-negative cancer (HR of death = 0.68, 95% CI = 0.53 to 0.88; P = .004). Five year-adjusted breast cancer survival for this group was improved with CPM vs without (88.5% vs 83.7%, difference = 4.8%). Although rates of contralateral breast cancer among young women with stages I-II disease undergoing CPM were independent of ER status, women with ER-positive tumors in the absence of prophylactic mastectomy also had a lower overall risk for contralateral breast cancer than women with ER-negative tumors (0.46% vs 0.90%, difference = 0.44%; P < .001).
Conclusions: CPM is associated with a small improvement in 5-year breast cancer-specific survival mainly in young women with early-stage ER-negative breast cancer. This effect is related to a higher baseline risk of contralateral breast cancer.
Figures
Comment in
-
Re: Population-based study of contralateral prophylactic mastectomy and survival outcomes of breast cancer patients.J Natl Cancer Inst. 2010 Sep 8;102(17):1371-2; author reply 1372-3. doi: 10.1093/jnci/djq298. Epub 2010 Aug 12. J Natl Cancer Inst. 2010. PMID: 20705935 No abstract available.
References
-
- Hartmann LC, Schaid DJ, Woods JE, et al. Efficacy of bilateral prophylactic mastectomy in women with a family history of breast cancer. N Engl J Med. 1999;340(2):77–84. - PubMed
-
- McDonnell SK, Schaid DJ, Myers JL, et al. Efficacy of contralateral prophylactic mastectomy in women with a personal and family history of breast cancer. J Clin Oncol. 2001;19(19):3938–3943. - PubMed
-
- Rebbeck TR, Friebel T, Lynch HT, et al. Bilateral prophylactic mastectomy reduces breast cancer risk in BRCA1 and BRCA2 mutation carriers: the PROSE Study Group. J Clin Oncol. 2004;22(6):1055–1062. - PubMed
-
- Meijers-Heijboer H, van Geel B, van Putten WL, et al. Breast cancer after prophylactic bilateral mastectomy in women with a BRCA1 or BRCA2 mutation. N Engl J Med. 2001;345(3):159–164. - PubMed
-
- Tuttle TM, Habermann EB, Grund EH, Morris TJ, Virnig BA. Increasing use of contralateral prophylactic mastectomy for breast cancer patients: a trend toward more aggressive surgical treatment. J Clin Oncol. 2007;25(33):5203–5209. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
