

Event rates, hospital utilization, and costs associated with major complications of diabetes: a multicountry comparative analysis
- PMID: 20186272
- PMCID: PMC2826379
- DOI: 10.1371/journal.pmed.1000236
Event rates, hospital utilization, and costs associated with major complications of diabetes: a multicountry comparative analysis
Abstract
Background: Diabetes imposes a substantial burden globally in terms of premature mortality, morbidity, and health care costs. Estimates of economic outcomes associated with diabetes are essential inputs to policy analyses aimed at prevention and treatment of diabetes. Our objective was to estimate and compare event rates, hospital utilization, and costs associated with major diabetes-related complications in high-, middle-, and low-income countries.
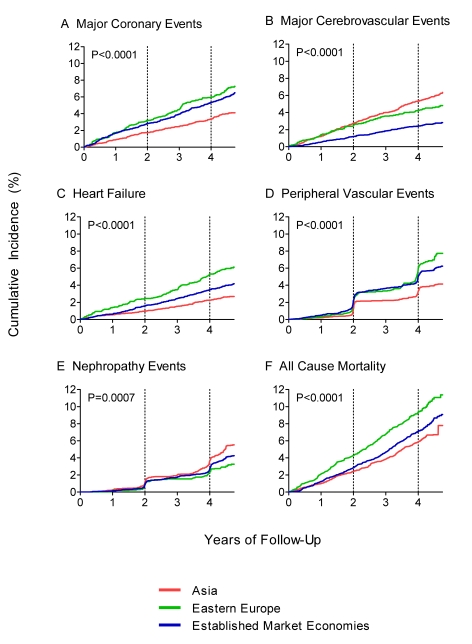
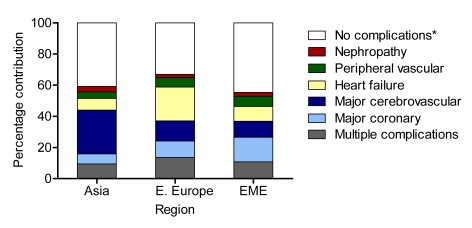
Methods and findings: Incidence and history of diabetes-related complications, hospital admissions, and length of stay were recorded in 11,140 patients with type 2 diabetes participating in the Action in Diabetes and Vascular Disease (ADVANCE) study (mean age at entry 66 y). The probability of hospital utilization and number of days in hospital for major events associated with coronary disease, cerebrovascular disease, congestive heart failure, peripheral vascular disease, and nephropathy were estimated for three regions (Asia, Eastern Europe, and Established Market Economies) using multiple regression analysis. The resulting estimates of days spent in hospital were multiplied by regional estimates of the costs per hospital bed-day from the World Health Organization to compute annual acute and long-term costs associated with the different types of complications. To assist, comparability, costs are reported in international dollars (Int$), which represent a hypothetical currency that allows for the same quantities of goods or services to be purchased regardless of country, standardized on purchasing power in the United States. A cost calculator accompanying this paper enables the estimation of costs for individual countries and translation of these costs into local currency units. The probability of attending a hospital following an event was highest for heart failure (93%-96% across regions) and lowest for nephropathy (15%-26%). The average numbers of days in hospital given at least one admission were greatest for stroke (17-32 d across region) and heart failure (16-31 d) and lowest for nephropathy (12-23 d). Considering regional differences, probabilities of hospitalization were lowest in Asia and highest in Established Market Economies; on the other hand, lengths of stay were highest in Asia and lowest in Established Market Economies. Overall estimated annual hospital costs for patients with none of the specified events or event histories ranged from Int$76 in Asia to Int$296 in Established Market Economies. All complications included in this analysis led to significant increases in hospital costs; coronary events, cerebrovascular events, and heart failure were the most costly, at more than Int$1,800, Int$3,000, and Int$4,000 in Asia, Eastern Europe, and Established Market Economies, respectively.
Conclusions: Major complications of diabetes significantly increase hospital use and costs across various settings and are likely to impose a high economic burden on health care systems.
Conflict of interest statement
PMC has received research grants from Servier. PG has received funding from the George Institute for the cost-effectiveness sub-study of the ADVANCE trial. AP reports receiving lecture fees from Servier, Pfizer, and Abbott and grant support from Pfizer, Servier, and Sanofi-Aventis. JC has received research grants from Servier, administered through the University of Sydney, as Co-Chief investigator for ADVANCE and has received lecture fees from Servier for speaking at scientific meetings. He has also received lecture fees from Pfizer and Daiichi and grant support from Servier. MW has received consulting fees from GlaxoSmithKline, AstraZeneca, and Pfizer, lecture fees from Pfizer, and grant support from Pfizer and Sanofi-Aventis. He has received lecture fees from Servier to present on the main results from ADVANCE (not those in this paper). He has also served on a steering committee for Roche. SBH has received lecture fees from Pfizer and Servier. JAS and AP are on the Editorial Board of
Figures
References
-
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–1053. - PubMed
-
- Gu K, Cowie CC, Harris MI. Mortality in adults with and without diabetes in a national cohort of the U. S. population, 1971–1993. Diabetes Care. 1998;21:1138–1145. - PubMed
-
- Narayan KM, Boyle JP, Thompson TJ, Sorensen SW, Williamson DF. Lifetime risk for diabetes mellitus in the United States. JAMA. 2003;290:1884–1890. - PubMed
-
- Selby JV, Ray GT, Zhang D, Colby CJ. Excess costs of medical care for patients with diabetes in a managed care population. Diabetes Care. 1997;20:1396–1402. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
