

Canadian Thoracic Society Asthma Management Continuum--2010 Consensus Summary for children six years of age and over, and adults
- PMID: 20186367
- PMCID: PMC2866209
- DOI: 10.1155/2010/827281
Canadian Thoracic Society Asthma Management Continuum--2010 Consensus Summary for children six years of age and over, and adults
Abstract
Background/objective: To integrate new evidence into the Canadian Asthma Management Continuum diagram, encompassing both pediatric and adult asthma.
Methods: The Canadian Thoracic Society Asthma Committee members, comprised of experts in pediatric and adult respirology, allergy and immunology, emergency medicine, general pediatrics, family medicine, pharmacoepidemiology and evidence-based medicine, updated the continuum diagram, based primarily on the 2008 Global Initiative for Asthma guidelines, and performed a focused review of literature pertaining to key aspects of asthma diagnosis and management in children six years of age and over, and adults.
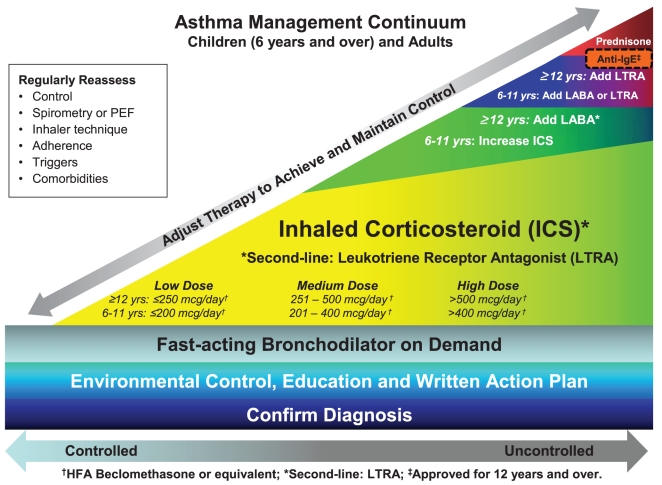
Results: In patients six years of age and over, management of asthma begins with establishing an accurate diagnosis, typically by supplementing medical history with objective measures of lung function. All patients and caregivers should receive self-management education, including a written action plan. Inhaled corticosteroids (ICS) remain the first-line controller therapy for all ages. When asthma is not controlled with a low dose of ICS, the literature supports the addition of long-acting beta2-agonists in adults, while the preferred approach in children is to increase the dose of ICS. Leukotriene receptor antagonists are acceptable as second-line monotherapy and as an alternative add-on therapy in both age groups. Antiimmunoglobulin E therapy may be of benefit in adults, and in children 12 years of age and over with difficult to control allergic asthma, despite high-dose ICS and at least one other controller.
Conclusions: The foundation of asthma management is establishing an accurate diagnosis based on objective measures (eg, spirometry) in individuals six years of age and over. Emphasis is placed on the similarities and differences between pediatric and adult asthma management approaches to achieve asthma control.
HISTORIQUE ET OBJECTIF :: Intégrer les nouvelles données probantes au diagramme du continuum canadien de prise en charge de l’asthme, englobant l’asthme à la fois chez les enfants et chez les adultes.
MÉTHODOLOGIE :: Les membres du comité sur l’asthme de la Société canadienne de thoracologie, composé d’experts en respirologie, en allergie et en immunologie chez les adultes et les enfants, en médecine d’urgence, en pédiatrie générale, en médecine de famille, en pharmacoépidémiologie et en médecine probante. Ils ont mis à jour le diagramme du continuum fondé principalement sur les lignes directrices de l’initiative mondiale 2008 sur l’asthme et procédé à une analyse bibliographique ciblée sur les principaux aspects du diagnostic et de la prise en charge de l’asthme chez les enfants de six ans et plus et les adultes.
RÉSULTATS :: Chez les patients de six ans et plus, la prise en charge de l’asthme commence par un diagnostic précis, généralement en complétant les antécédents médicaux de mesures objectives de la fonction pulmonaire. Tous les patients et les soignants devraient être informés des modes d’autogestion, y compris un plan d’action écrit. Les corticoïdes en aérosol (CEA) demeurent le traitement de contrôle de première ligne à tout âge. Lorsque l’asthme ne se contrôle pas au moyen d’une faible dose de CEA, les publications étayent l’ajout d’un bêta2-agoniste de longue durée chez les adultes, tandis que, chez les enfants, on favorise l’accroissement de la dose de CEA. Les antagonistes des récepteurs des leucotriènes sont acceptables comme monothérapie de deuxième ligne et comme autre traitement d’appoint dans les deux groupes d’âge. La thérapie à l’anti-immunoglobuline E peut être bénéfique aux adultes ainsi qu’aux enfants de 12 ans et plus éprouvant de la difficulté à contrôler l’asthme allergique malgré de forte doses de CEA et au moins un autre traitement de contrôle.
CONCLUSIONS :: Les assises de la prise en charge de l’asthme consistent à poser un diagnostic exact fondé sur des mesures objectives (p. ex., spirométrie) chez les personnes de six ans et plus. On s’attarde sur les similarités et les différences entre les démarches de prise en charge de l’asthme chez les enfants et chez les adultes afin de contrôler l’asthme.
Figures
References
-
- Lemiere C, Bai T, Balter M, et al. Adult Asthma Consensus Guidelines Update 2003. Can Respir J. 2004;11(Suppl A):9A–18A. - PubMed
-
- Expert Panel Report 3 (EPR 3): Guidelines for the Diagnosis and Management of Asthma. 2007. Bethseda, Maryland, National Heart, Lung, and Blood Institute, National Institutes of Health, No. 08-4051 (prepublication copy).
-
- British Guideline on the Management of Asthma: A national clinical guideline. Scottish Intercollegiate Guidelines Network (SIGN); British Thoracic Society; 2008
-
- Global Initiative for Asthma (GINA) Global Strategy for Asthma Management and Prevention, 2008. <http://www.ginasthma.com/GuidelinesResources.asp?l1=2&l2=0> (Accessed November, 2009).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
