

Admissions to Canadian hospitals for acute asthma: a prospective, multicentre study
- PMID: 20186368
- PMCID: PMC2866213
- DOI: 10.1155/2010/178549
Admissions to Canadian hospitals for acute asthma: a prospective, multicentre study
Abstract
Background: Asthma exacerbations constitute one of the most common causes of emergency department (ED) attendance in most developed countries. While severe asthma often requires hospitalization, variability in admission practices has been observed.
Objective: To describe the factors associated with admission to Canadian hospitals for acute asthma after ED treatment.
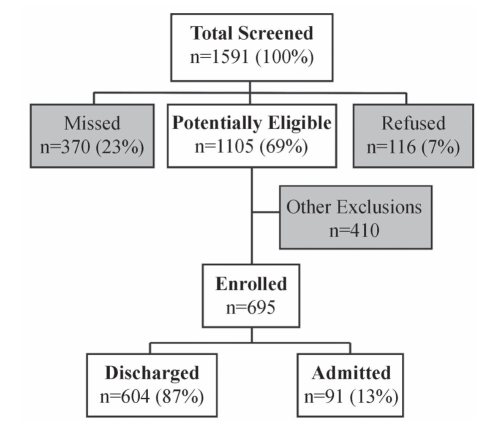
Methods: Subjects 18 to 55 years of age treated for acute asthma in 20 Canadian EDs prospectively underwent a structured ED interview (n=695) and telephone interview two weeks later.
Results: The median age of the patients was 30 years, and the majority were women (62.8%). The admission rate was 13.1% (95% CI 10.7% to 15.8%). Admitted patients were older, more often receiving oral or inhaled corticosteroids at presentation, and more frequently receiving systemic corticosteroids and magnesium sulphate in the ED. Similar proportions received beta-2 agonists and/or ipratropium bromide within 1 h of arrival. On multivariable analyses, factors associated with admission included age, previous admission in the past two years, more than eight beta-2 agonist puffs in the past 24 h, a Canadian Triage and Acuity Score of 1 to 2, a respiratory rate of greater than 22 breaths/min and an oxygen saturation of less than 95%.
Conclusion: The admission rate for acute asthma from these Canadian EDs was lower than reported in other North American studies. The present study provides insight into practical factors associated with admission for acute asthma and highlights the importance of history and asthma severity markers on ED decision making. Further efforts to standardize ED management and expedite admission decision-making appear warranted.
HISTORIQUE :: Les exacerbations de l’asthme constituent l’une des principales causes de visites au département d’urgence (DU) dans la plupart des pays industrialisés. Bien que l’asthme grave exige souvent une hospitalisation, on a observé une variabilité dans les pratiques d’admission.
OBJECTIF :: Décrire les facteurs liés à l’admission dans un hôpital canadien en raison d’un asthme aigu après un traitement au DU.
MÉTHODOLOGIE :: Des sujets de 18 à 55 ans traités en raison d’un asthme aigu dans 20 DU canadiens ont passé une entrevue prospective au DU (n=695), suivie d’une entrevue téléphonique deux semaines plus tard.
RÉSULTATS :: Les patients avaient un âge médian de 30 ans et étaient majoritairement des femmes (62,8 %). Le taux d’admission s’élevait à 13,1 % (95 % IC 10,7 % à 15,8 %). Les patients hospitalisés étaient plus âgés, recevaient plus souvent des corticoïdes par voie orale ou en aérosol et on leur donnait plus souvent des corticoïdes et du sulfure de magnésium systémiques au DU. Des proportions similaires recevaient des bêta2-agonistes ou du bromure d’ipratropium dans l’heure suivant leur arrivée au DU. D’après les analyses multivariées, les facteurs associés à l’admission incluaient l’âge, l’hospitalisation au cours des deux années précédentes, plus de huit bouffées de bêta2-agonistes au cours des 24 heures précédentes, un indice canadien de triage et d’acuité de 1 à 2, une fréquence respiratoire supérieure à 22 respirations/min et une saturation en oxygène inférieure à 95 %.
CONCLUSION :: Le taux d’hospitalisation découlant d’un asthme aigu à partir de ces DU canadiens était inférieur à celui déclaré dans d’autres études nord-américaines. La présente étude fournit un aperçu des facteurs pratiques associés à l’hospitalisation découlant d’un asthme aigu et fait ressortir l’importance des antécédents et des marqueurs de gravité de l’asthme dans la prise de décision au DU. D’autres mesures pour normaliser la prise en charge au DU et accélérer la prise de décision au sujet de l’hospitalisation semblent s’imposer.
Comment in
-
Asthma in the emergency room in Canada.Can Respir J. 2010 Jan-Feb;17(1):13-4. doi: 10.1155/2010/752569. Can Respir J. 2010. PMID: 20186366 Free PMC article. No abstract available.
References
-
- O’Byrne PM. Airway inflammation and the pathogenesis of asthma. Can Respir J. 1994;1:189–95.
-
- Chapman KR, Ernst P, Grenville A, Dewland P, Zimmerman S. Control of asthma in Canada: Failure to achieve guideline targets. Can Respir J. 2001;8:35A–40A. (Abst) - PubMed
-
- American Lung Association Trends in asthma morbidity and mortality. 2007.
-
- Weiss KB, Sullivan SD, Lyttle CS. Trends in the cost of illness for asthma in the United States, 1985–1994. J Allergy Clin Immun. 2000;106:493–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
