

When should ulcerative colitis patients undergo colectomy for dysplasia? Mismatch between patient preferences and physician recommendations
- PMID: 20186940
- PMCID: PMC2927807
- DOI: 10.1002/ibd.21233
When should ulcerative colitis patients undergo colectomy for dysplasia? Mismatch between patient preferences and physician recommendations
Abstract
Background: If dysplasia is found on biopsies during surveillance colonoscopy for ulcerative colitis (UC), many experts recommend colectomy given the substantial risk of synchronous colon cancer. The objective was to learn if UC patients' perceptions of their colon cancer risk and if their preferences for elective colectomy match with physicians' recommendations if dysplasia was found.
Methods: A self-administered written survey included 199 patients with UC for at least 8 years (mean age 49 years, 52% female) who were recruited from Dartmouth-Hitchcock (n = 104) and the University of Chicago (n = 95). The main outcome was the proportion of patients who disagree with physicians' recommendations for colectomy because of dysplasia.
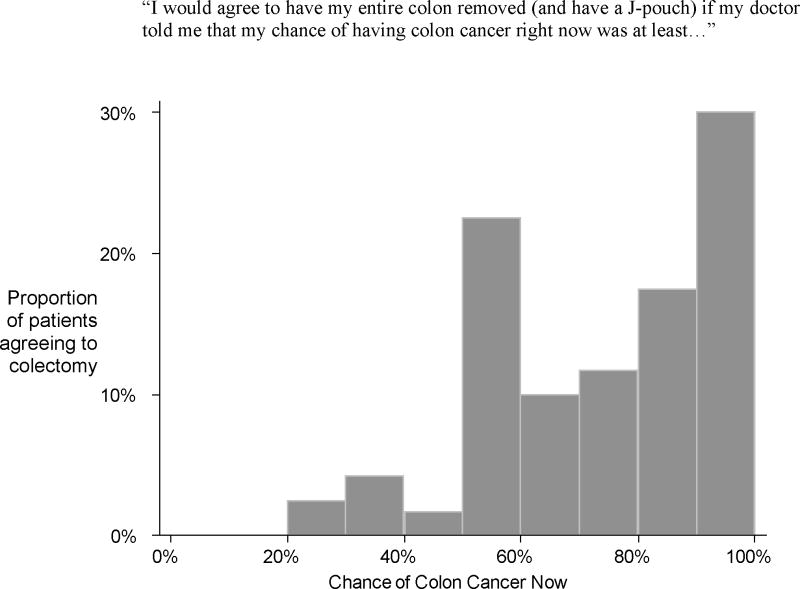
Results: Almost all respondents recognized that UC raised their chance of getting colon cancer. In all, 74% thought it was "unlikely" or "very unlikely" to get colon cancer within the next 10 years and they quantified this risk to be 23%; 60% of patients would refuse a physician's recommendation for elective colectomy if dysplasia was detected, despite being told that they had a 20% risk of having cancer now. On average, these patients would only agree to colectomy if their risk of colon cancer "right now" were at least 73%.
Conclusions: UC patients recognize their increased risk of colon cancer and undergo frequent surveillance to reduce their risk. Nonetheless, few seem prepared to follow standard recommendations for elective colectomy if dysplasia is found. This may reflect the belief that surveillance alone is sufficient to reduce their colon cancer risk or genuine disagreement about when it is worth undergoing colectomy.
Figures
References
-
- Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults (update): American College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol. 2004;99:1371–1385. - PubMed
-
- Thomas T, Abrams KA, Robinson RJ, et al. Meta-analysis: cancer risk of low-grade dysplasia in chronic ulcerative colitis. Aliment Pharmacol Ther. 2007;25:657–668. - PubMed
-
- Ullman T, Croog V, Harpaz N, et al. Progression of flat low-grade dysplasia to advanced neoplasia in patients with ulcerative colitis. Gastroenterology. 2003;125:1311–1319. - PubMed
-
- Itzkowitz SH, Present DH. Consensus conference: colorectal cancer screening and surveillance in inflammatory bowel disease. Inflamm Bowel Dis. 2005;11:314–321. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical