

Clinical outcomes of systemic therapy for patients with deep fibromatosis (desmoid tumor)
- PMID: 20187095
- PMCID: PMC2925106
- DOI: 10.1002/cncr.25089
Clinical outcomes of systemic therapy for patients with deep fibromatosis (desmoid tumor)
Abstract
Background: In the current study, the authors examined the outcomes of patients with desmoid tumors who received systemic therapy at a single institution to provide a basis for the examination of newer agents.
Methods: Records of patients with desmoid tumors who were treated with chemotherapy at the study institution were reviewed. The activity of nonsteroidal anti-inflammatory drugs was not addressed. Patients without measurable disease and those receiving therapy could not be documented, and those receiving prophylactic therapy were excluded.
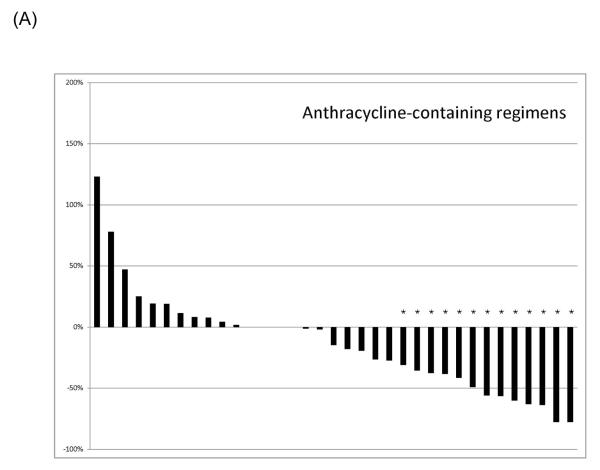
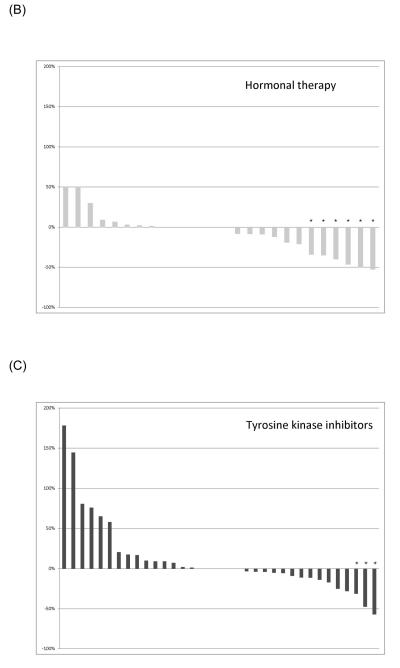
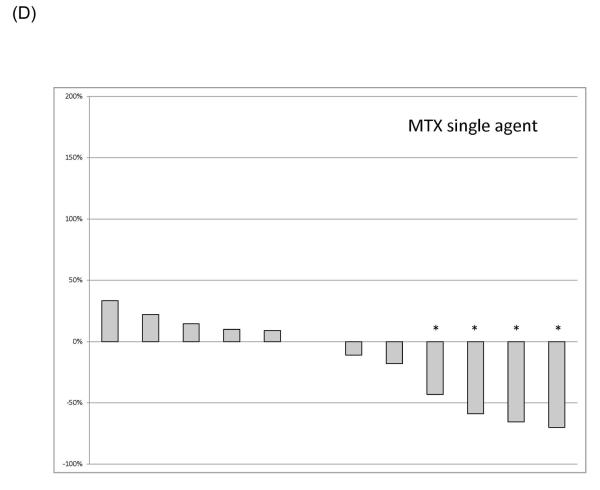
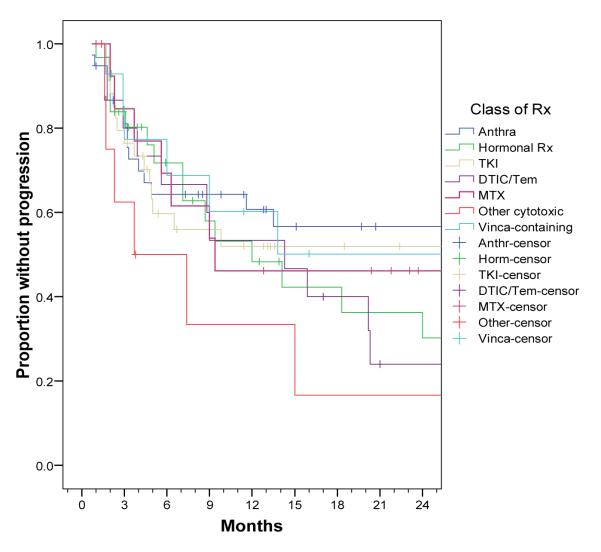
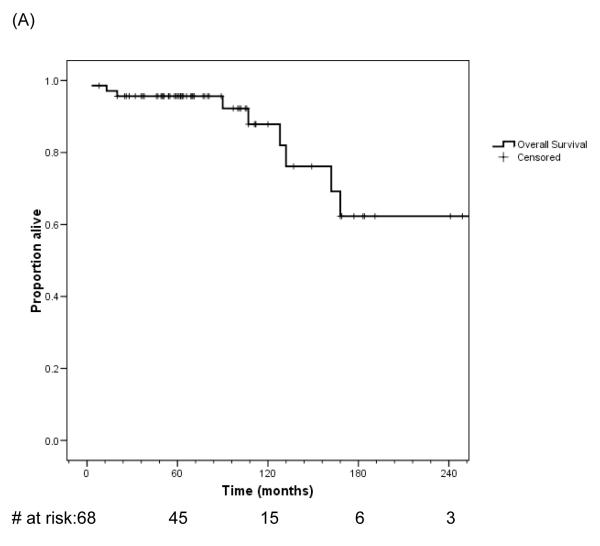
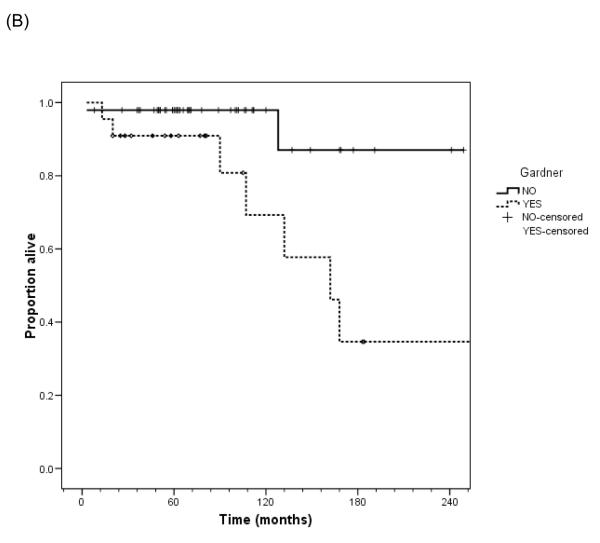
Results: A total of 68 patients received 157 lines of therapy. At the time of last follow-up, 9 patients had died, 7 of progressive disease. The cohort was 62% female, with a median age of 32.5 years. Approximately 32% of the patients had Gardner syndrome. The median follow-up was 63 months, and patients received a median of 2 lines of therapy. An intra-abdominal primary tumor location was the most common (44%). The greatest Response Evaluation Criteria in Solid Tumors (RECIST) response rate was observed with anthracyclines and hormonal therapy and the lowest response was noted with single-agent dacarbazine/temozolomide or tyrosine kinase inhibitors, principally imatinib. On multivariate analysis, macroscopic nodular morphology and the presence of Gardner syndrome were the only tumor factors found to be associated with a greater time to disease progression.
Conclusions: Compared with other agents, antiestrogens and anthracycline-containing regimens appear to be associated with a higher radiological response rate against desmoid tumors. Systemic therapy can be successful in patients with desmoid tumors, and is a viable option in lieu of morbid or disabling surgery.
(c) 2010 American Cancer Society.
Figures
References
-
- Alman BA, Pajerski ME, Diaz-Cano S, Corboy K, Wolfe HJ. Aggressive fibromatosis (desmoid tumor) is a monoclonal disorder. Diagn Mol Pathol. 1997;6(2):98–101. - PubMed
-
- Hosalkar HS, Torbert JT, Fox EJ, Delaney TF, Aboulafia AJ, Lackman RD. Musculoskeletal desmoid tumors. J Am Acad Orthop Surg. 2008;16(4):188–98. - PubMed
-
- Nieuwenhuis MH, De Vos Tot Nederveen Cappel W, Botma A, Nagengast FM, Kleibeuker JH, Mathus-Vliegen EM, et al. Desmoid tumors in a dutch cohort of patients with familial adenomatous polyposis. Clin Gastroenterol Hepatol. 2008;6(2):215–9. - PubMed
-
- Bertario L, Russo A, Sala P, Varesco L, Giarola M, Mondini P, et al. Multiple approach to the exploration of genotype-phenotype correlations in familial adenomatous polyposis. J Clin Oncol. 2003;21(9):1698–707. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
