

Effect of blood flow on double inversion recovery vessel wall MRI of the peripheral arteries: quantitation with T2 mapping and comparison with flow-insensitive T2-prepared inversion recovery imaging
- PMID: 20187182
- PMCID: PMC2921169
- DOI: 10.1002/mrm.22227
Effect of blood flow on double inversion recovery vessel wall MRI of the peripheral arteries: quantitation with T2 mapping and comparison with flow-insensitive T2-prepared inversion recovery imaging
Erratum in
- Magn Reson Med. 2010 Nov;64(5):1540
Abstract
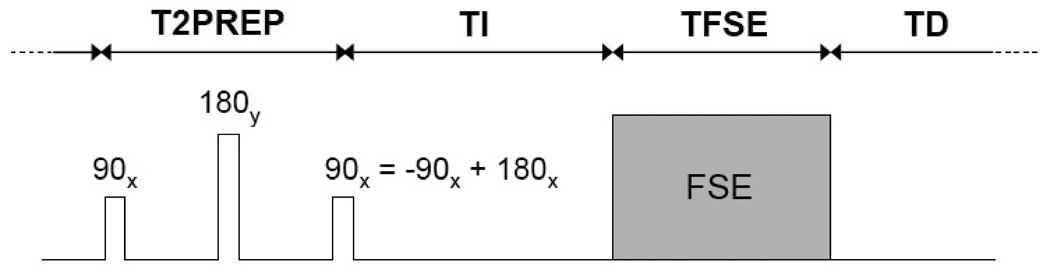
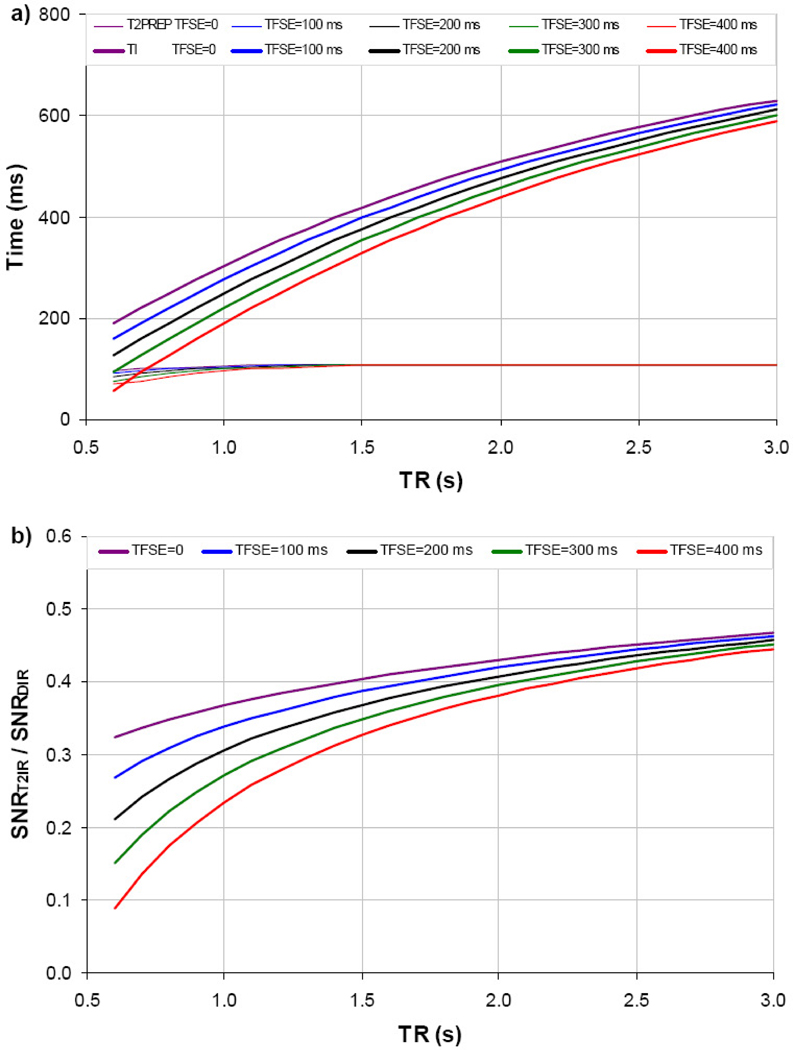
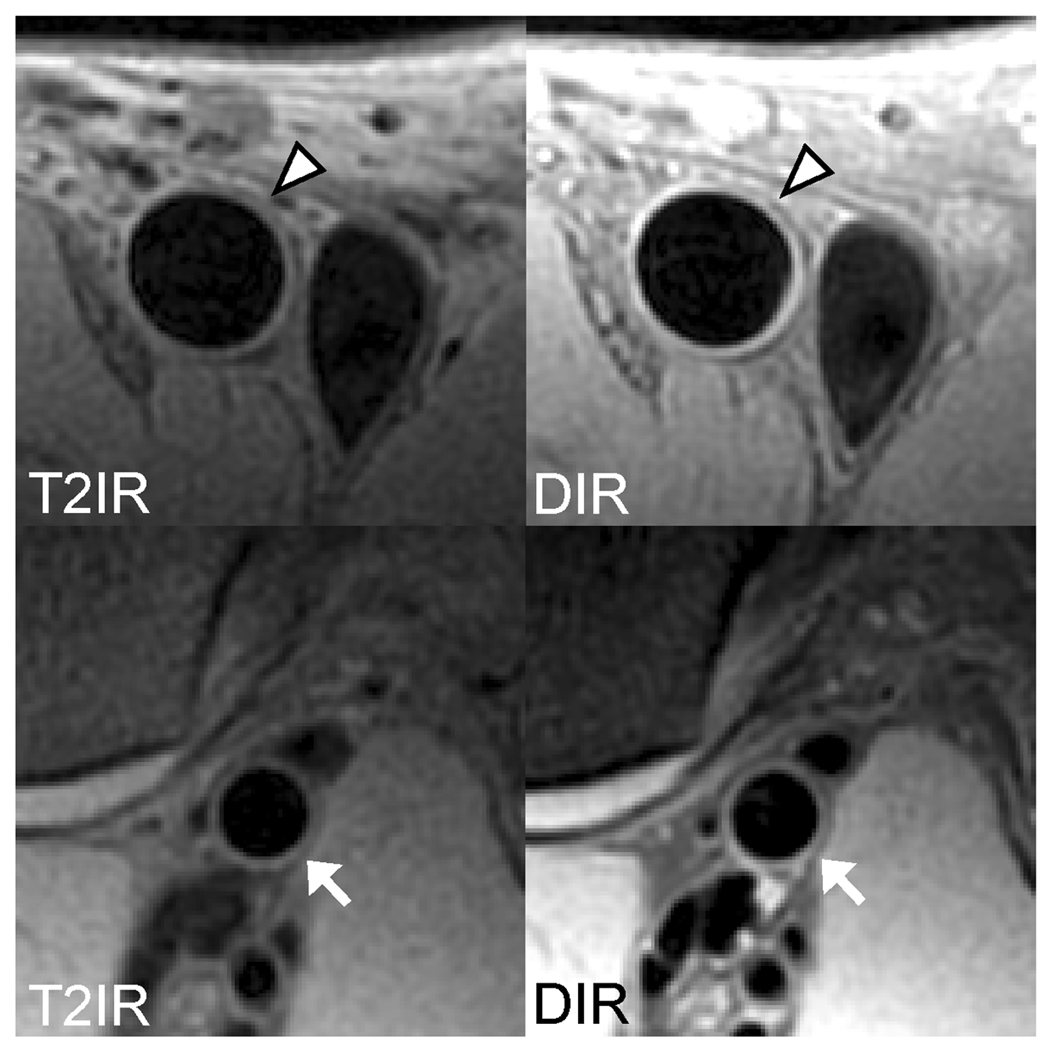
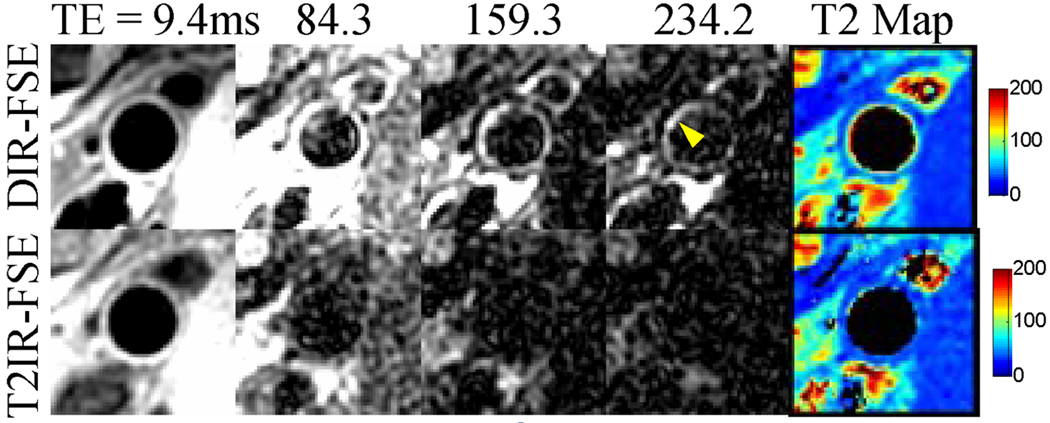
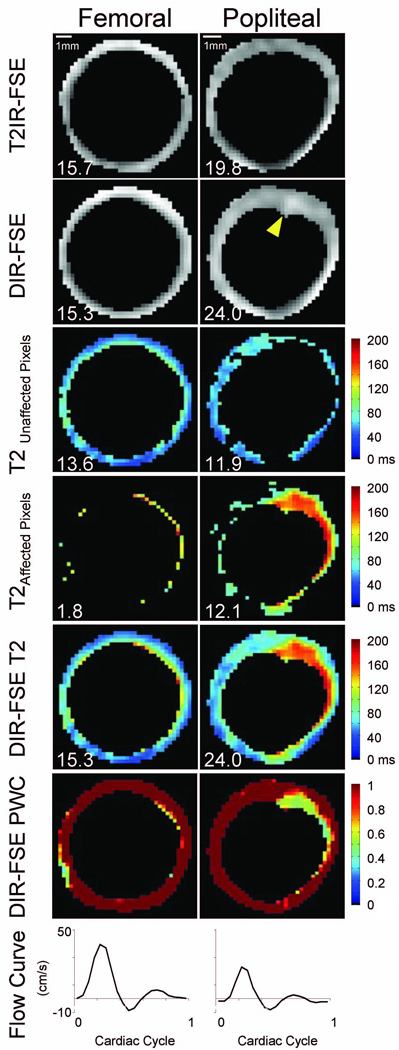
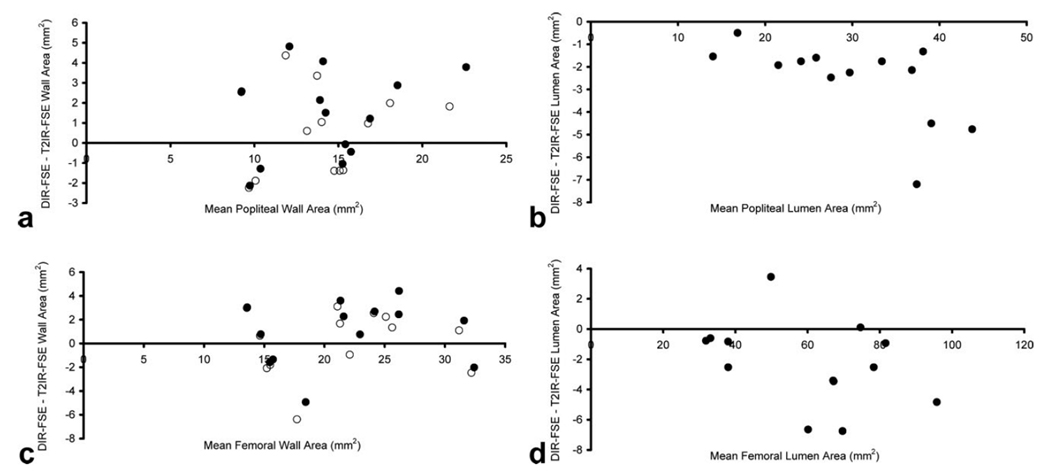
Blood suppression in the lower extremities using flow-reliant methods such as double inversion recovery may be problematic due to slow blood flow. T(2) mapping using fast spin echo (FSE) acquisition was utilized to quantitate the effectiveness of double inversion recovery blood suppression in 13 subjects and showed that 25 +/- 12% of perceived vessel wall pixels in the popliteal arteries contained artifactual blood signal. To overcome this problem, a flow-insensitive T(2)-prepared inversion recovery sequence was implemented and optimal timing parameters were calculated for FSE acquisition. Black blood vessel wall imaging of the popliteal and femoral arteries was performed using two-dimensional T(2)-prepared inversion recovery-FSE in the same 13 subjects. Comparison with two-dimensional double inversion recovery-FSE showed that T(2)-prepared inversion recovery-FSE reduced wall-mimicking blood artifacts that inflated double inversion recovery-FSE vessel wall area measurements in the popliteal artery.
(c) 2010 Wiley-Liss, Inc.
Figures
References
-
- Amarenco P, Cohen A, Tzourio C, Bertrand B, Hommel M, Besson G, Chauvel C, Touboul PJ, Bousser MG. Atherosclerotic disease of the aortic arch and the risk of ischemic stroke. N Engl J Med. 1994;331(22):1474–1479. - PubMed
-
- Smilde TJ, van den Berkmortel FW, Boers GH, Wollersheim H, de Boo T, van Langen H, Stalenhoef AF. Carotid and femoral artery wall thickness and stiffness in patients at risk for cardiovascular disease, with special emphasis on hyperhomocysteinemia. Arterioscler Thromb Vasc Biol. 1998;18(12):1958–1963. - PubMed
-
- Demarco JK, Rutt BK, Clarke SE. Carotid plaque characterization by magnetic resonance imaging: review of the literature. Top Magn Reson Imaging. 2001;12(3):205–217. - PubMed
-
- Underhill HR, Yuan C, Zhao XQ, Kraiss LW, Parker DL, Saam T, Chu B, Takaya N, Liu F, Polissar NL, Neradilek B, Raichlen JS, Cain VA, Waterton JC, Hamar W, Hatsukami TS. Effect of rosuvastatin therapy on carotid plaque morphology and composition in moderately hypercholesterolemic patients: a high-resolution magnetic resonance imaging trial. Am Heart J. 2008;155(3):584, e581–e588. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
