

Intensity-modulated radiation therapy (IMRT) vs. 3D conformal radiotherapy (3DCRT) in locally advanced rectal cancer (LARC): dosimetric comparison and clinical implications
- PMID: 20187944
- PMCID: PMC2845593
- DOI: 10.1186/1748-717X-5-17
Intensity-modulated radiation therapy (IMRT) vs. 3D conformal radiotherapy (3DCRT) in locally advanced rectal cancer (LARC): dosimetric comparison and clinical implications
Abstract
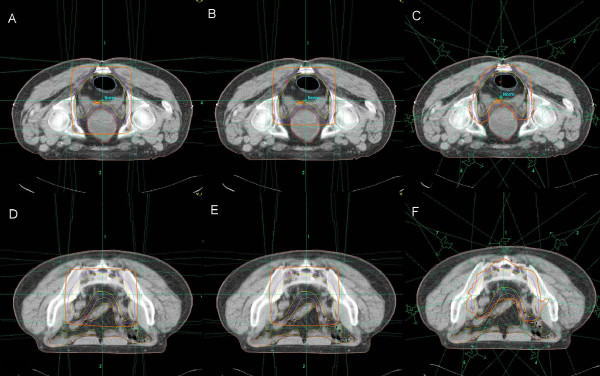
Purpose: To compare target dose distribution, comformality, normal tissue avoidance, and irradiated body volume (IBV) in 3DCRT using classic anatomical landmarks (c3DCRT), 3DCRT fitting the PTV (f3DCRT), and intensity-modulated radiation therapy (IMRT) in patients with locally advanced rectal cancer (LARC).
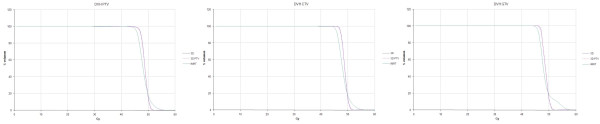
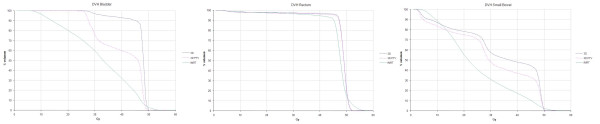
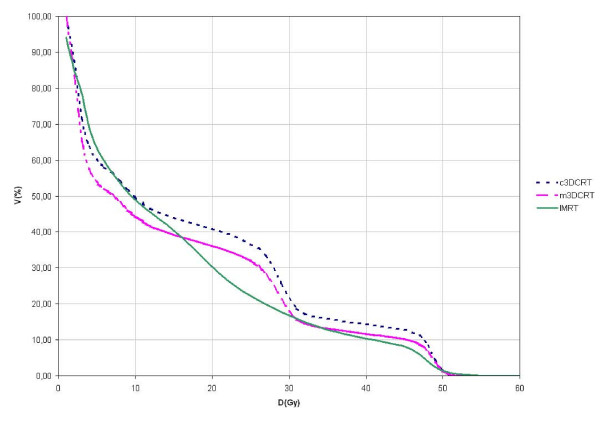
Materials and methods: Fifteen patients with LARC underwent c3DCRT, f3DCRT, and IMRT planning. Target definition followed the recommendations of the ICRU reports No. 50 and 62. OAR (SB and bladder) constraints were D5 < or = 50 Gy and Dmax < 55 Gy. PTV dose prescription was defined as PTV95 > or = 45 Gy and PTVmin > or = 35 Gy. Target coverage was evaluated with the D95, Dmin, and Dmax. Target dose distribution and comformality was evaluated with the homogeneity indices (HI) and Conformity Index (CI). Normal tissue avoidance of OAR was evaluated with the D5 and V40. IBV at 5 Gy (V5), 10 Gy (V10), and 20 Gy (V20) were calculated.
Results: The mean GTV95, CTV95, and PTV95 doses were significantly lower for IMRT plans. Target dose distribution was more inhomogeneous after IMRT planning and 3DCRTplans had significantly lower CI. The V40 and D5 values for OAR were significantly reduced in the IMRT plans .V5 was greater for IMRT than for f3DCRT planning (p < 0.05) and V20 was smaller for IMRT plans(p < 0.05).
Conclusions: IMRT planning improves target conformity and decreases irradiation of the OAR at the expense of increased target heterogeneity. IMRT planning increases the IBV at 5 Gy or less but decreases the IBV at 20 Gy or more.
Figures
References
-
- Bosset JF, Calais G, Daban A, Berger C, Radosevic-Jelic L, Maingon P. Preoperative chemoradiotherapy versus preoperative radiotherapy in rectal cancer patients: assessment of acute toxicity and treatment compliance. Report of the 22921 randomised trial conducted by the EORTC Radiotherapy Group. Eur J Cancer. 2004;40(2):219–224. doi: 10.1016/j.ejca.2003.09.032. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
