

Safety and efficacy of thrombectomy in patients undergoing primary percutaneous coronary intervention for acute ST elevation MI: a meta-analysis of randomized controlled trials
- PMID: 20187958
- PMCID: PMC2838805
- DOI: 10.1186/1471-2261-10-10
Safety and efficacy of thrombectomy in patients undergoing primary percutaneous coronary intervention for acute ST elevation MI: a meta-analysis of randomized controlled trials
Abstract
Background: Clinical trials comparing thrombectomy devices with conventional percutaneous coronary interventions (PCI) in patients with acute ST elevation myocardial infarction (STEMI) have produced conflicting results. The objective of our study was to systematically evaluate currently available data comparing thrombectomy followed by PCI with conventional PCI alone in patients with acute STEMI.
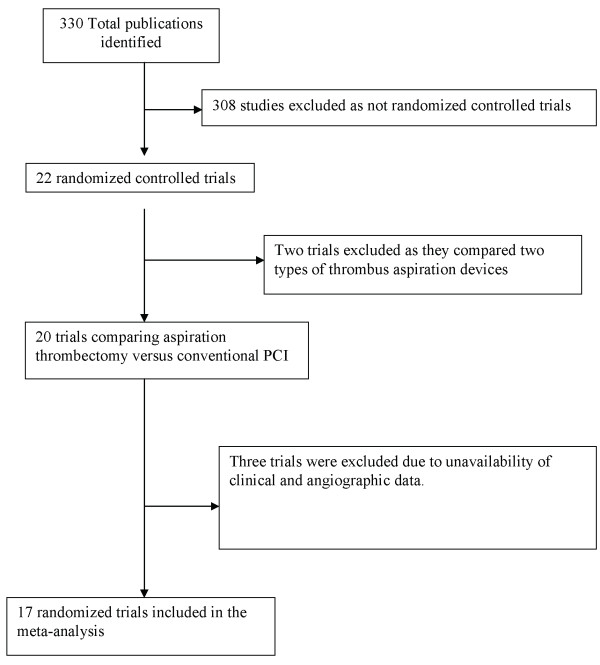
Methods: Seventeen randomized trials (n = 3,909 patients) of thrombectomy versus PCI were included in this meta-analysis. We calculated the summary odds ratios for mortality, stroke, post procedural myocardial blush grade (MBG), thrombolysis in myocardial infarction (TIMI) grade flow, and post procedural ST segment resolution (STR) using random-effects and fixed-effects models.
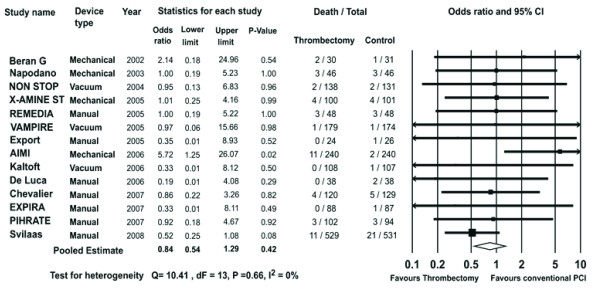
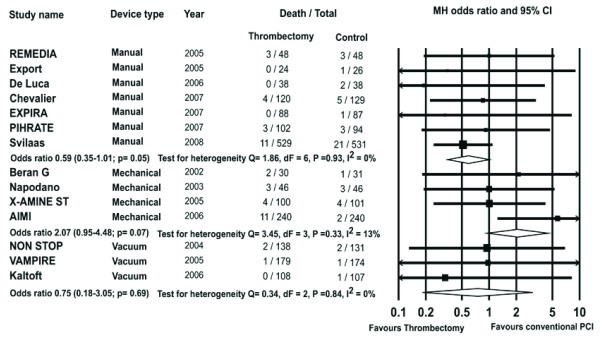
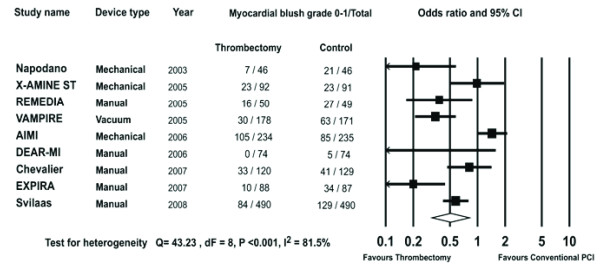
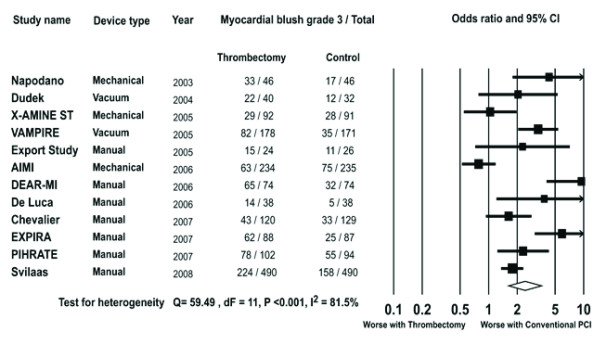
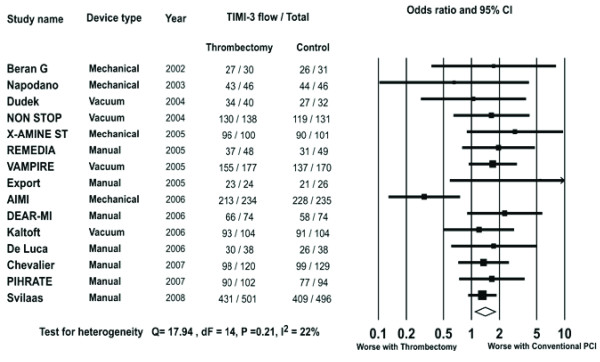
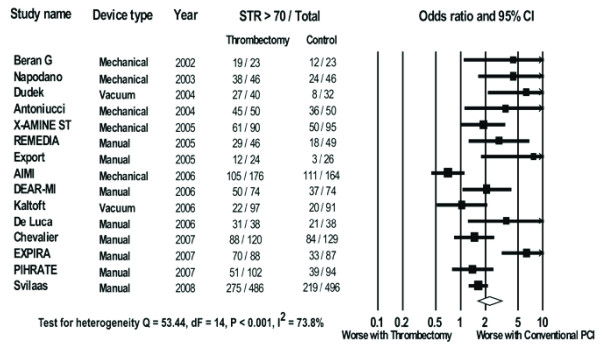
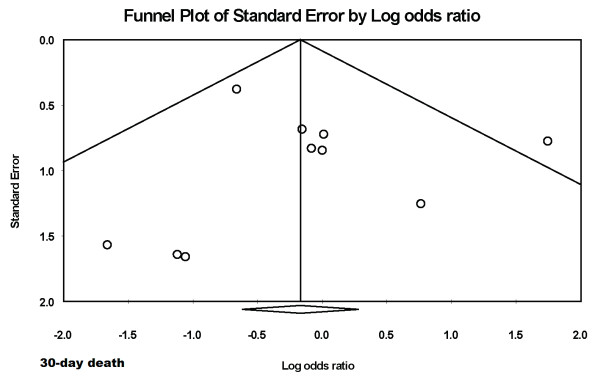
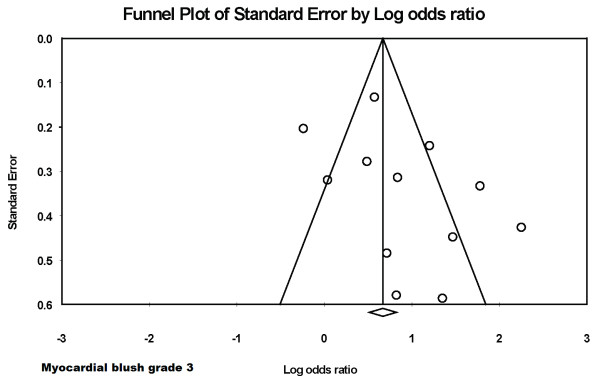
Results: There was no difference in risk of 30-day mortality (44/1914 vs. 50/1907, OR 0.84, 95% CI 0.54-1.29, P = 0.42) among patients randomized to thrombectomy, compared with conventional PCI. Thrombectomy was associated with a significantly greater likelihood of TIMI 3 flow (1616/1826 vs. 1533/1806, OR 1.41, P = 0.007), MBG 3 (730/1526 vs. 486/1513, OR 2.42, P < 0.001), STR (923/1500 vs. 715/1494, OR 2.30, P < 0.001), and with a higher risk of stroke (14/1403 vs. 3/1413, OR 2.88, 95% CI 1.06-7.85, P = 0.04). Outcomes differed significantly between different device classes with a trend towards lower mortality with manual aspiration thrombectomy (MAT) (21/949 vs.36/953, OR 0.59, 95% CI 0.35-1.01, P = 0.05), whereas mechanical devices showed a trend towards higher mortality (20/416 vs.10/418, OR 2.07, 95% CI 0.95-4.48, P = 0.07).
Conclusions: Thrombectomy devices appear to improve markers of myocardial perfusion in patients undergoing primary PCI, with no difference in overall 30-day mortality but an increased likelihood of stroke. The clinical benefits of thrombectomy appear to be influenced by the device type with a trend towards survival benefit with MAT and worsening outcome with mechanical devices.
Figures
References
-
- De Luca G, van't Hof AWJ, Ottervanger JP, Hoorntje JCA, Gosselink ATM, Dambrink J-HE, Zijlstra F, de Boer M-J, Suryapranata H. Unsuccessful reperfusion in patients with ST-segment elevation myocardial infarction treated by primary angioplasty. American Heart Journal. 2005;150(3):557–562. doi: 10.1016/j.ahj.2004.10.044. - DOI - PubMed
-
- Gibson CM, Cannon CP, Murphy SA, Ryan KA, Mesley R, Marble SJ, McCabe CH, Werf F Van De, Braunwald E. Relationship of TIMI myocardial perfusion grade to mortality after administration of thrombolytic drugs. Circulation. 2000;101(2):125–130. - PubMed
-
- Burzotta F, Testa L, Giannico F, Biondi-Zoccai GGL, Trani C, Romagnoli E, Mazzari M, Mongiardo R, Siviglia M, Niccoli G. Adjunctive devices in primary or rescue PCI: A meta-analysis of randomized trials. International Journal of Cardiology. 2008;123(3):313–321. doi: 10.1016/j.ijcard.2006.12.018. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
