

MR imaging of high-grade brain tumors using endogenous protein and peptide-based contrast
- PMID: 20188197
- PMCID: PMC2856810
- DOI: 10.1016/j.neuroimage.2010.02.050
MR imaging of high-grade brain tumors using endogenous protein and peptide-based contrast
Abstract
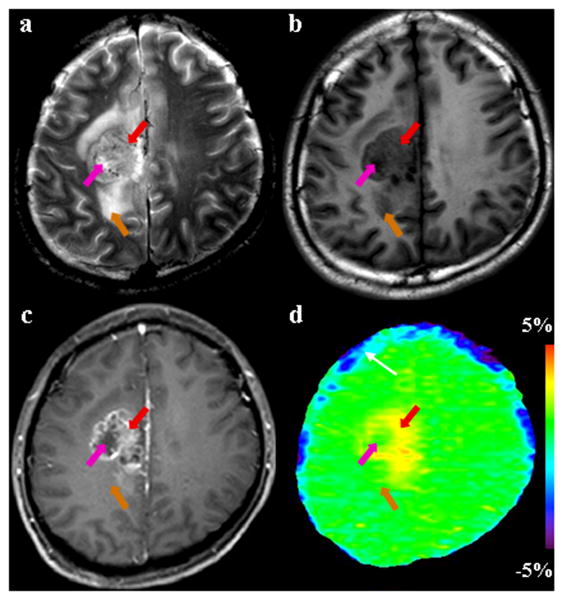
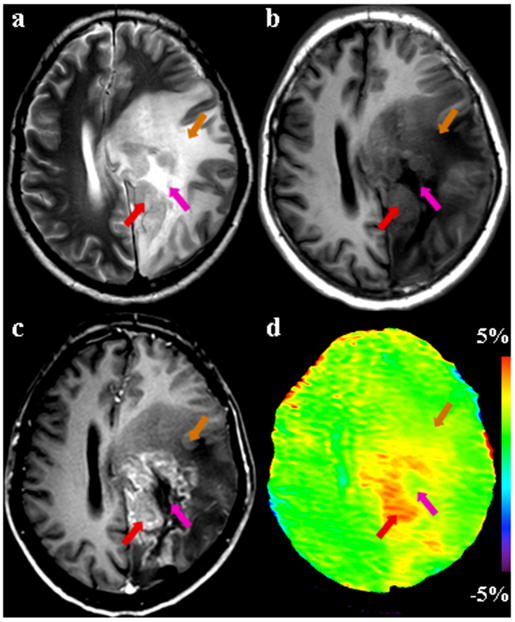
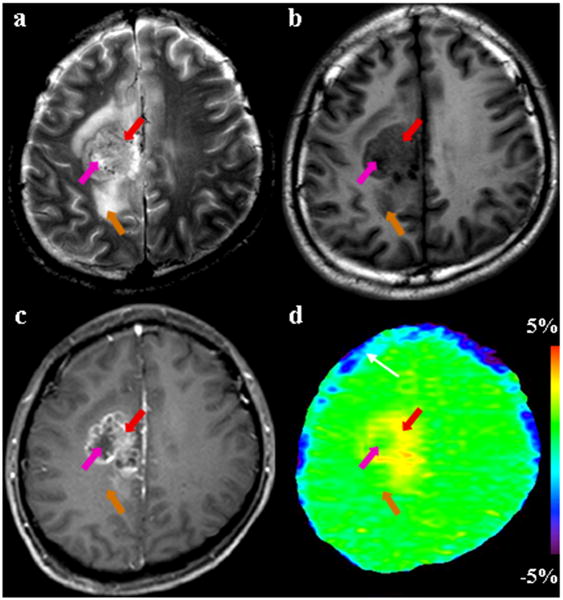
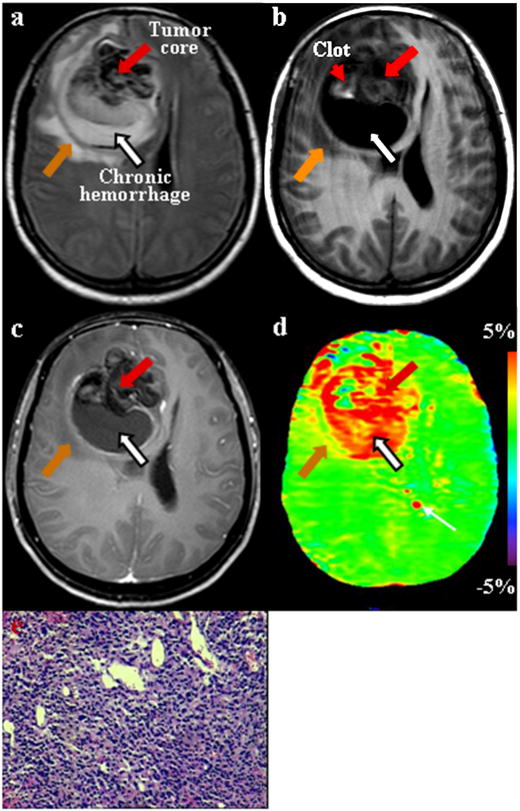
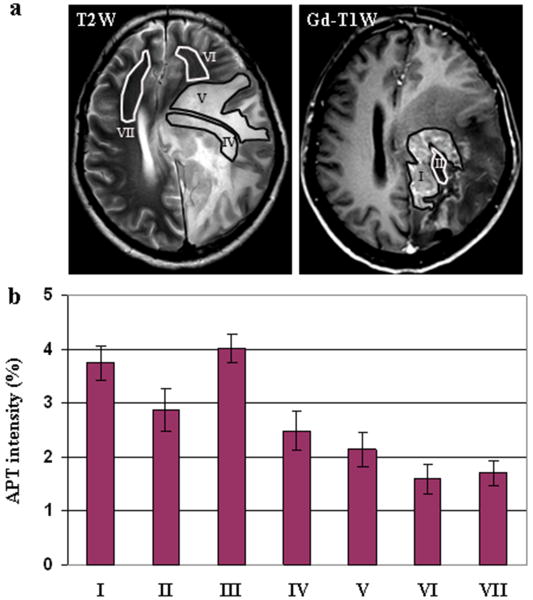
Amide proton transfer (APT) imaging is a novel MRI technique, in which the amide protons of endogenous proteins and peptides are irradiated to accomplish indirect detection using the bulk water signal. In this paper, the APT approach was added to a standard brain MRI protocol at 3T, and twelve patients with high-grade gliomas confirmed by histopathology were scanned. It is shown that all tumors, including one with minor gadolinium enhancement, showed heterogeneous hyperintensity on the APT images. The average APT signal intensities of the viable tumor cores were significantly higher than those of peritumoral edema and normal-appearing white matter (P<0.001). The average APT signal intensities were significantly lower in the necrotic regions than in the viable tumor cores (P=0.004). The APT signal intensities of the cystic cavities were similar to those of the viable tumor cores (P>0.2). The initial results show that APT imaging at the protein and peptide level may enhance non-invasive identification of tissue heterogeneity in high-grade brain tumors.
Copyright 2010 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Three-dimensional amide proton transfer MR imaging of gliomas: Initial experience and comparison with gadolinium enhancement.J Magn Reson Imaging. 2013 Nov;38(5):1119-28. doi: 10.1002/jmri.24067. Epub 2013 Feb 25. J Magn Reson Imaging. 2013. PMID: 23440878 Free PMC article.
-
Practical data acquisition method for human brain tumor amide proton transfer (APT) imaging.Magn Reson Med. 2008 Oct;60(4):842-9. doi: 10.1002/mrm.21712. Magn Reson Med. 2008. PMID: 18816868 Free PMC article.
-
Whole-brain amide proton transfer (APT) and nuclear overhauser enhancement (NOE) imaging in glioma patients using low-power steady-state pulsed chemical exchange saturation transfer (CEST) imaging at 7T.J Magn Reson Imaging. 2016 Jul;44(1):41-50. doi: 10.1002/jmri.25108. Epub 2015 Dec 10. J Magn Reson Imaging. 2016. PMID: 26663561 Free PMC article.
-
An evidence-based approach to evaluate the accuracy of amide proton transfer-weighted MRI in characterization of gliomas.Medicine (Baltimore). 2019 Mar;98(10):e14768. doi: 10.1097/MD.0000000000014768. Medicine (Baltimore). 2019. PMID: 30855481 Free PMC article.
-
Amide Proton Transfer-Chemical Exchange Saturation Transfer Imaging of Intracranial Brain Tumors and Tumor-like Lesions: Our Experience and a Review.Diagnostics (Basel). 2023 Feb 28;13(5):914. doi: 10.3390/diagnostics13050914. Diagnostics (Basel). 2023. PMID: 36900058 Free PMC article. Review.
Cited by
-
Amide proton transfer imaging of the breast at 3 T: establishing reproducibility and possible feasibility assessing chemotherapy response.Magn Reson Med. 2013 Jul;70(1):216-24. doi: 10.1002/mrm.24450. Epub 2012 Aug 20. Magn Reson Med. 2013. PMID: 22907893 Free PMC article.
-
Review and consensus recommendations on clinical APT-weighted imaging approaches at 3T: Application to brain tumors.Magn Reson Med. 2022 Aug;88(2):546-574. doi: 10.1002/mrm.29241. Epub 2022 Apr 22. Magn Reson Med. 2022. PMID: 35452155 Free PMC article. Review.
-
Chemical exchange saturation transfer MRI to assess cell death in breast cancer xenografts at 7T.Oncotarget. 2018 Jul 31;9(59):31490-31501. doi: 10.18632/oncotarget.25844. eCollection 2018 Jul 31. Oncotarget. 2018. PMID: 30140385 Free PMC article.
-
3D Amide Proton Transfer Weighted Brain Tumor Imaging With Compressed SENSE: Effects of Different Acceleration Factors.Front Neurosci. 2022 May 26;16:876587. doi: 10.3389/fnins.2022.876587. eCollection 2022. Front Neurosci. 2022. PMID: 35692419 Free PMC article.
-
MRI detection of bacterial brain abscesses and monitoring of antibiotic treatment using bacCEST.Magn Reson Med. 2018 Aug;80(2):662-671. doi: 10.1002/mrm.27180. Epub 2018 Mar 25. Magn Reson Med. 2018. PMID: 29577382 Free PMC article.
References
-
- Aime S, Barge A, Delli Castelli D, Fedeli F, Mortillaro A, Nielsen FU, Terreno E. Paramagnetic Lanthanide(III) complexes as pH-sensitive chemical exchange saturation transfer (CEST) contrast agents for MRI applications. Magn Reson Med. 2002;47:639–648. - PubMed
-
- Brandsma D, Stalpers L, Taal W, Sminia P, van den Bent MJ. Clinical features, mechanisms, and management of pseudoprogression in malignant gliomas. Lancet Oncol. 2008;9:453–461. - PubMed
-
- Broome DR. Nephrogenic systemic fibrosis associated with gadolinium based contrast agents: A summary of the medical literature reporting. Eur J Radiol. 2008;66:230–234. - PubMed
-
- Burger PC, Dubois PJ, Schold SCJ, Smith KRJ, Odom GL, Crafts DC, Giangaspero F. Computerized tomographic and pathologic studies of the untreated, quiescent, and recurrent glioblastoma multiforme. J Neurosurg. 1983;58:159–169. - PubMed
-
- Catalaa I, Henry R, Dillon WP, Graves EE, McKnight TR, Lu Y, Vigneron DB, Nelson SJ. Perfusion, diffusion and spectroscopy values in newly diagnosed cerebral gliomas. NMR Biomed. 2006;19:463–475. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
