

Comparative effectiveness of prostate cancer surgical treatments: a population based analysis of postoperative outcomes
- PMID: 20188381
- PMCID: PMC2866516
- DOI: 10.1016/j.juro.2009.12.021
Comparative effectiveness of prostate cancer surgical treatments: a population based analysis of postoperative outcomes
Erratum in
- J Urol. 2010 Aug;184(2):808
Abstract
Purpose: Enthusiasm for laparoscopic surgical approaches to prostate cancer treatment has grown despite limited evidence of improved outcomes compared with open radical prostatectomy. We compared laparoscopic prostatectomy with or without robotic assistance vs open radical prostatectomy in terms of postoperative outcomes and subsequent cancer directed therapy.
Materials and methods: Using a population based cancer registry linked with Medicare claims we identified men 66 years old or older with localized prostate cancer who underwent radical prostatectomy from 2003 to 2005. Outcome measures were general medical/surgical complications and mortality within 90 days after surgery, genitourinary/bowel complications within 365 days, radiation therapy and/or androgen deprivation therapy within 365 days and length of hospital stay.
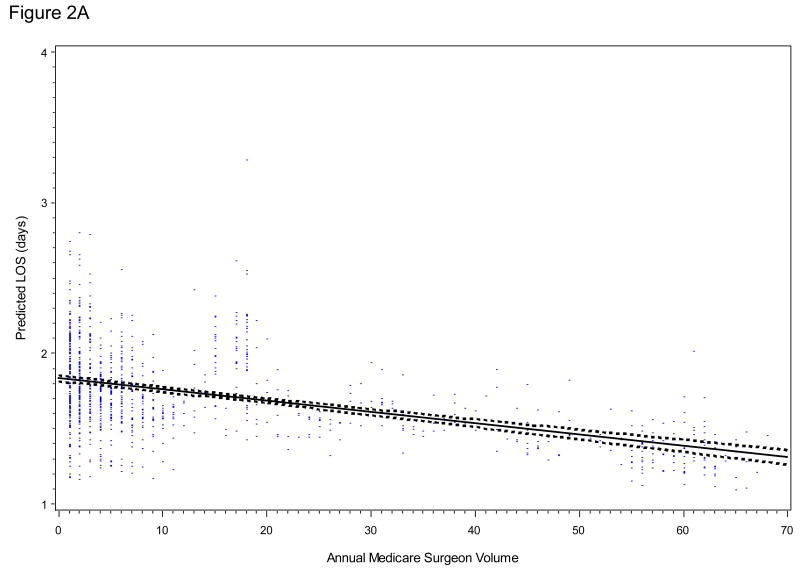
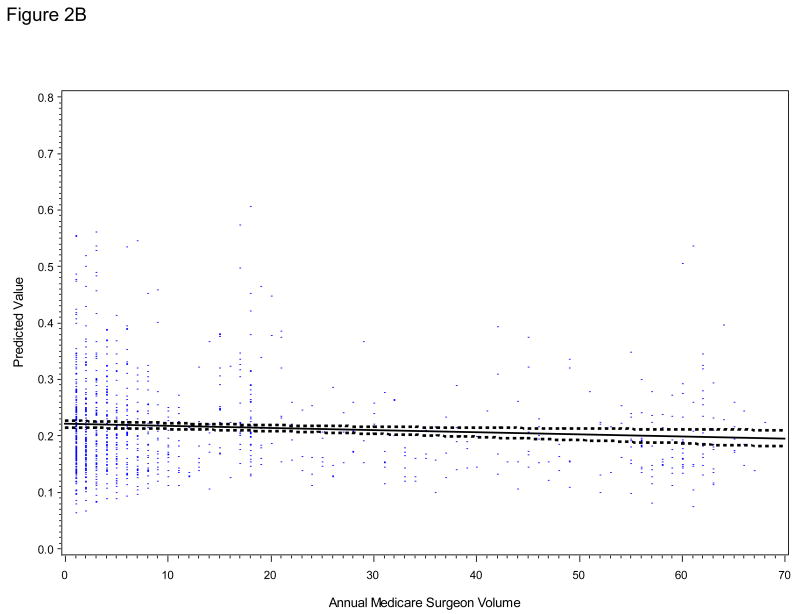
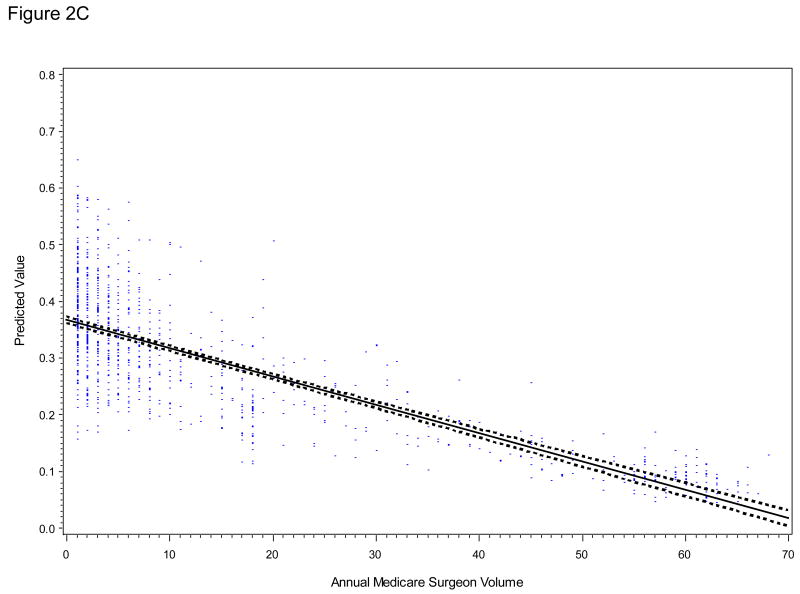
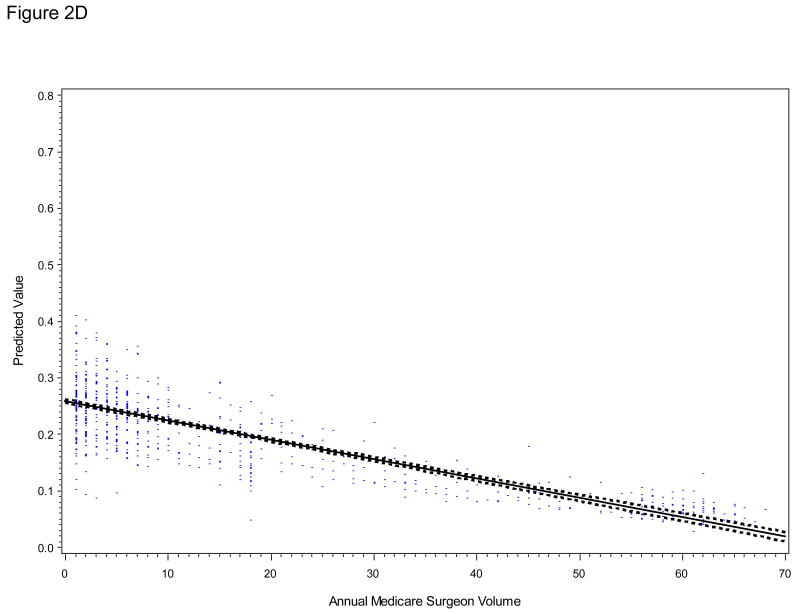
Results: Of the 5,923 men 18% underwent laparoscopic radical prostatectomy. Adjusting for patient and tumor characteristics, there were no differences in the rate of general medical/surgical complications (OR 0.93 95% CI 0.77-1.14) or genitourinary/bowel complications (OR 0.96 95% CI 0.76-1.22), or in postoperative radiation and/or androgen deprivation (OR 0.80 95% CI 0.60-1.08). Laparoscopic prostatectomy was associated with a 35% shorter hospital stay (p <0.0001) and a lower bladder neck/urethral obstruction rate (OR 0.74, 95% CI 0.58-0.94). In laparoscopic cases surgeon volume was inversely associated with hospital stay and the odds of any genitourinary/bowel complication.
Conclusions: Laparoscopic prostatectomy and open radical prostatectomy have similar rates of postoperative morbidity and additional treatment. Men considering prostate cancer surgery should understand the expected benefits and risks of each technique to facilitate decision making and set realistic expectations.
Copyright (c) 2010 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Editorial comment.J Urol. 2010 Apr;183(4):1372. doi: 10.1016/j.juro.2009.12.123. Epub 2010 Feb 25. J Urol. 2010. PMID: 20188380 No abstract available.
-
Re: Comparative effectiveness of prostate cancer surgical treatments: a population based analysis of postoperative outcomes: W. T. Lowrance, E. B. Elkin, L. M. Jacks, D. S. Yee, T. L. Jang, V. P. Laudone, B. D. Guillonneau, P. T. Scardino and J. A. Eastham J Urol 2010; 183: 1366-1372.J Urol. 2010 Oct;184(4):1573-4; author reply 1574. doi: 10.1016/j.juro.2010.06.034. Epub 2010 Aug 21. J Urol. 2010. PMID: 20732691 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71. - PubMed
-
- Guillonneau B, Vallancien G. Laparoscopic radical prostatectomy: the Montsouris experience. J Urol. 2000;163:418. - PubMed
-
- Schuessler WW, Kavoussi LR, Clayman RV, et al. Laparoscopic radical prostatectomy: initial case report. J Urol. 1992;147:246A. - PubMed
-
- Schuessler WW, Schulam PG, Clayman RV, et al. Laparoscopic radical prostatectomy: initial short-term experience. Urology. 1997;50:854. - PubMed
-
- Abbou CC, Hoznek A, Salomon L, et al. Remote laparoscopic radical prostatectomy carried out with a robot. Report of a case. Prog Urol. 2000;10:520. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
