

Dissecting aneurysms of the distal segment of the posterior inferior cerebellar arteries: clinical presentation and management
- PMID: 20190207
- PMCID: PMC7963947
- DOI: 10.3174/ajnr.A2014
Dissecting aneurysms of the distal segment of the posterior inferior cerebellar arteries: clinical presentation and management
Abstract
Background and purpose: Dissecting aneurysms of the distal segment of the PICA are rare. The purpose of this study was to evaluate the clinical presentations, imaging features, treatment options, and clinical outcomes of dissecting PICA aneurysms.
Materials and methods: Six patients with dissecting aneurysms in the distal segments of PICA were found in the database of a single medical center, from November 1996 to December 2008, and retrospectively evaluated. Treatment mode and follow-up clinical outcomes were analyzed.
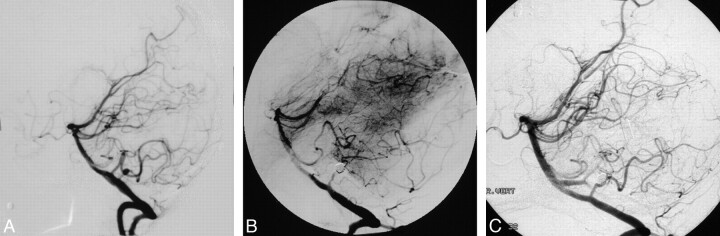
Results: Five patients with dissecting PICA aneurysms presented with acute intracranial hemorrhage and 1 patient presented with a large mass from an intramural hematoma. All 5 patients with intracranial hemorrhage were treated with endovascular occlusion of both the dissecting PICA aneurysm and the distal parent artery. The patient with the intramural hematoma underwent surgical trapping with end-to-end anastomosis. In 1 patient, the dissecting aneurysm recurred twice within a 5 year 3 month period, despite endovascular occlusion of both the aneurysm and the parent artery. The clinical outcome postprocedure was excellent in all patients, without permanent neurologic complication.
Conclusions: For the endovascular treatment of dissecting aneurysms in the distal PICA segments, we recommend occlusion of both the dissecting aneurysm and the parent artery to avoid leaving the point of initial intimal tear untreated. All of our patients had excellent clinical outcomes; however, our experience with recanalization illustrates the need for close follow-up of patients.
Figures


Similar articles
-
Endovascular treatment of isolated posterior inferior cerebellar artery dissecting aneurysms: parent artery occlusion or selective coiling?Clin Neuroradiol. 2014 Sep;24(3):255-61. doi: 10.1007/s00062-013-0247-5. Epub 2013 Aug 4. Clin Neuroradiol. 2014. PMID: 23913020 Clinical Trial.
-
Dissecting distal cerebellar artery aneurysms: options beyond a parent vessel sacrifice.Neurosurg Rev. 2020 Apr;43(2):771-780. doi: 10.1007/s10143-019-01119-y. Epub 2019 May 29. Neurosurg Rev. 2020. PMID: 31144196
-
Onyx embolization in distal dissecting posterior inferior cerebellar artery aneurysms.J Neurointerv Surg. 2016 May;8(5):501-6. doi: 10.1136/neurintsurg-2014-011622. Epub 2015 Apr 2. J Neurointerv Surg. 2016. PMID: 25838199
-
Endovascular parent vessel sacrifice in ruptured dissecting vertebral and posterior inferior cerebellar artery aneurysms: clinical outcomes and review of the literature.J Neurointerv Surg. 2016 Aug;8(8):796-801. doi: 10.1136/neurintsurg-2015-011732. Epub 2015 Aug 3. J Neurointerv Surg. 2016. PMID: 27417905 Review.
-
[Dissecting aneurysm of the posterior inferior cerebellar artery--studied by serial angiography].No Shinkei Geka. 2001 Nov;29(11):1057-62. No Shinkei Geka. 2001. PMID: 11758313 Review. Japanese.
Cited by
-
Aneurysms of the medullary segments of the posterior-inferior cerebellar artery: considerations on treatment strategy and clinical outcome.Neurol Sci. 2013 Apr;34(4):529-36. doi: 10.1007/s10072-012-1095-9. Epub 2012 Apr 22. Neurol Sci. 2013. PMID: 22526768
-
Endovascular Embolization with n-Butyl Cyanoacrylate for Ruptured Distal Posterior Inferior Cerebellar Artery Dissecting Aneurysm.Asian J Neurosurg. 2023 Sep 22;18(3):651-655. doi: 10.1055/s-0042-1757432. eCollection 2023 Sep. Asian J Neurosurg. 2023. PMID: 38152529 Free PMC article.
-
Endovascular treatment of ruptured distal posterior inferior cerebellar artery aneurysms: report of 11 cases.Afr Health Sci. 2014 Mar;14(1):89-93. doi: 10.4314/ahs.v14i1.14. Afr Health Sci. 2014. PMID: 26060463 Free PMC article.
-
Dissecting aneurysms of posterior communicating artery itself: anatomical, diagnostic, clinical, and therapeutical considerations.Neuroradiology. 2013 Sep;55(9):1103-12. doi: 10.1007/s00234-013-1212-3. Epub 2013 Jun 21. Neuroradiology. 2013. PMID: 23793861
-
The re-anastomosis end-to-end bypass technique: a comprehensive review of the technical characteristics and surgical experience.Neurosurg Rev. 2019 Sep;42(3):619-629. doi: 10.1007/s10143-018-1036-z. Epub 2018 Sep 25. Neurosurg Rev. 2019. PMID: 30255374 Review.
References
-
- Kanou Y, Arita K, Kurisu K, et al. . Dissecting aneurysm of the peripheral posterior inferior cerebellar artery. Acta Neurochir (Wien) 2000;142:1151–56 - PubMed
-
- Tamano Y, Ujiie H, Hori T. Postoperative hemorrhage due to normal pressure hyperperfusion breakthrough after a trapping of VA-PICA dissecting aneurysm [in Japanese]. No Shinkei Geka 2000;28:257–62 - PubMed
-
- Anxionnat R, de Melo Neto JF, Bracard S, et al. . Treatment of hemorrhagic intracranial dissections. Neurosurgery 2003;53:289–300; discussion 300–01 - PubMed
-
- Yamakawa H, Kaku Y, Yoshimura S, et al. . Two cases of dissecting aneurysm of the distal posterior inferior cerebellar artery: possible involvement of segmental mediolytic arteriopathy in the pathogenesis. Clin Neurol Neurosurg 2005;107:117–22 - PubMed
-
- Tawk RG, Bendok BR, Qureshi AI, et al. . Isolated dissections and dissecting aneurysms of the posterior inferior cerebellar artery: topic and literature review. Neurosurg Rev 2002;26:180–87 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical