

Sex-specific responses to stroke
- PMID: 20190872
- PMCID: PMC2827821
- DOI: 10.2217/fnl.09.66
Sex-specific responses to stroke
Abstract
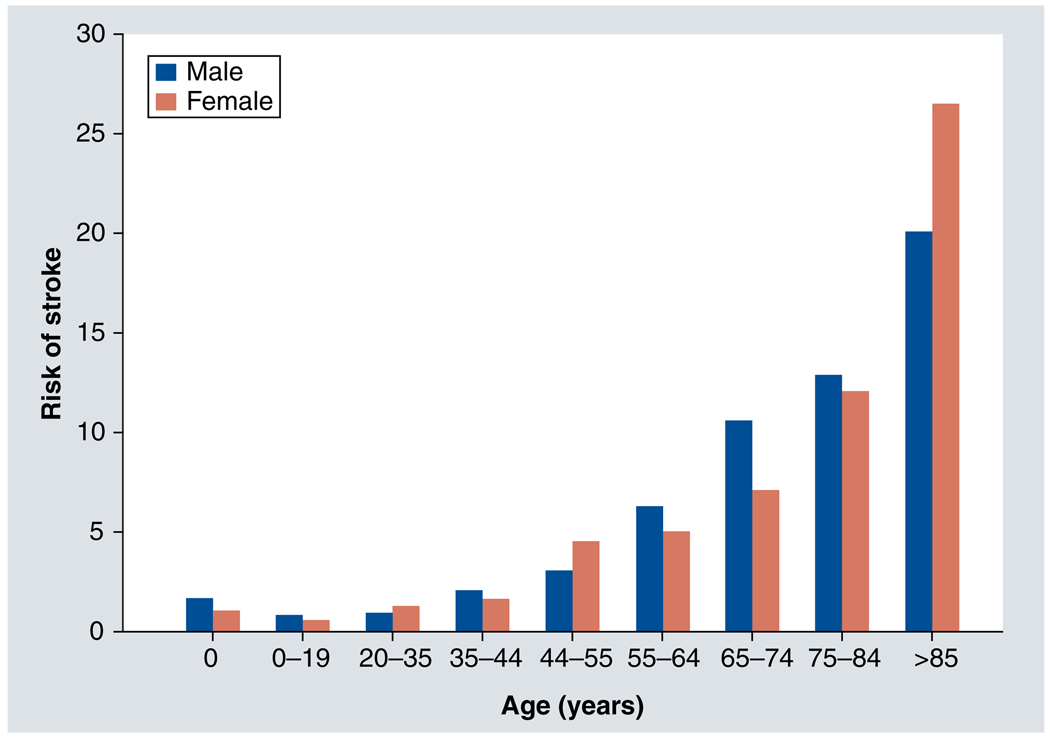
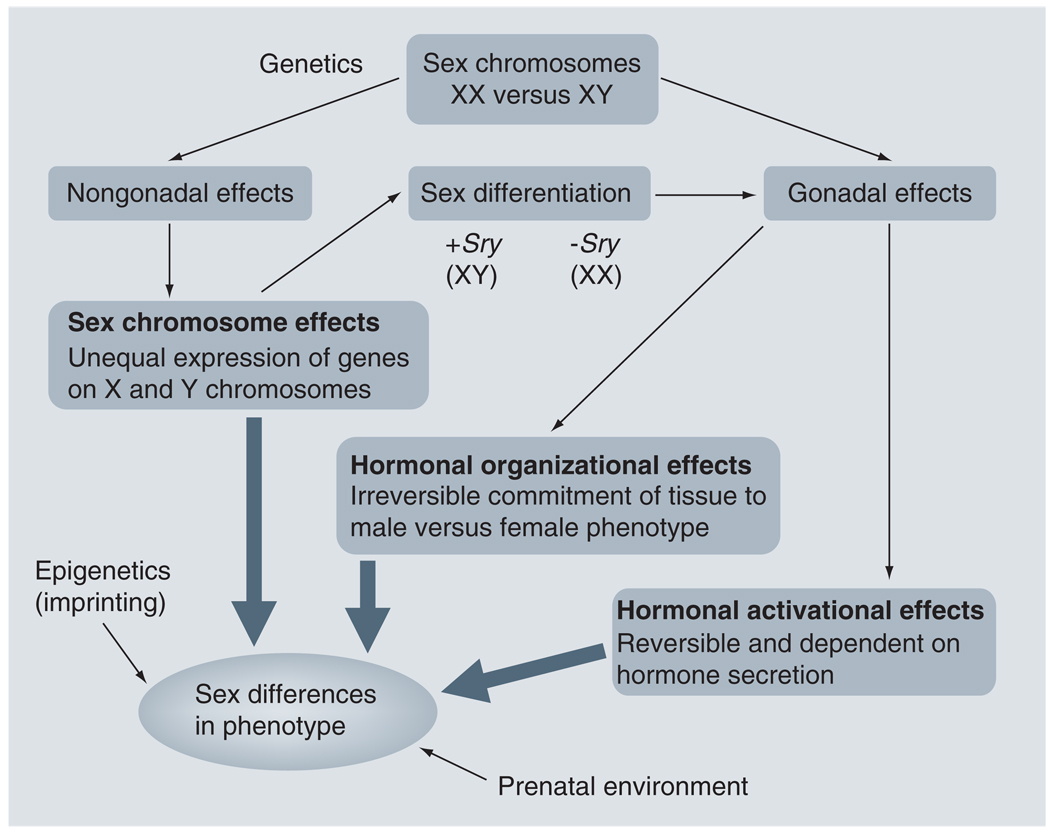
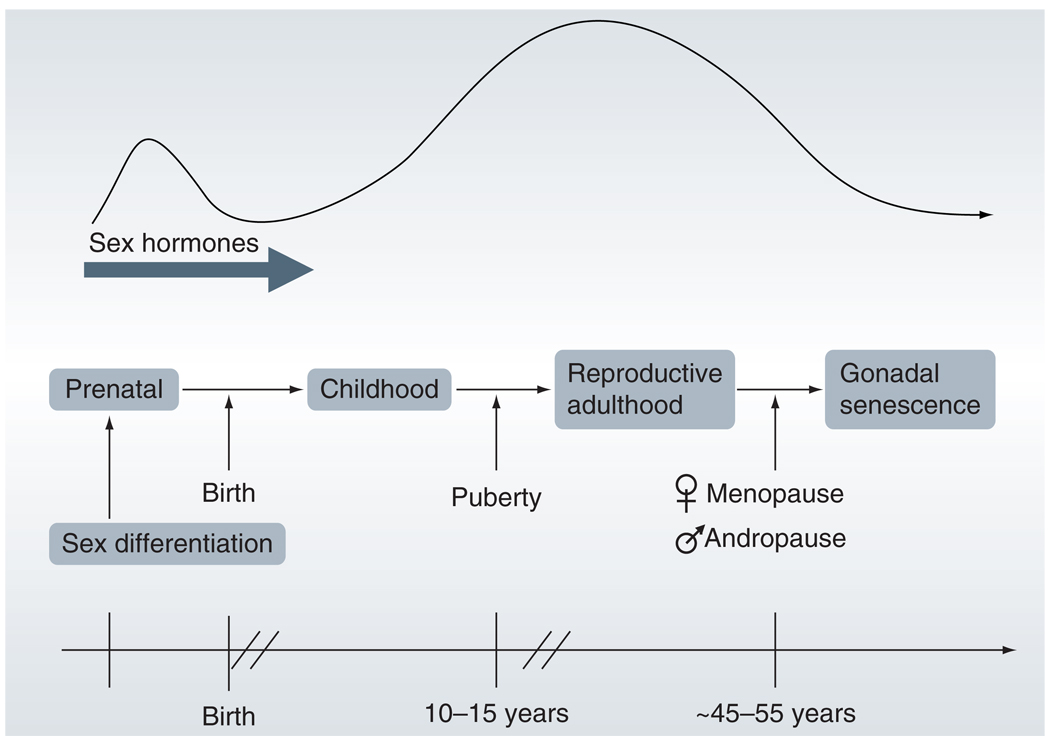
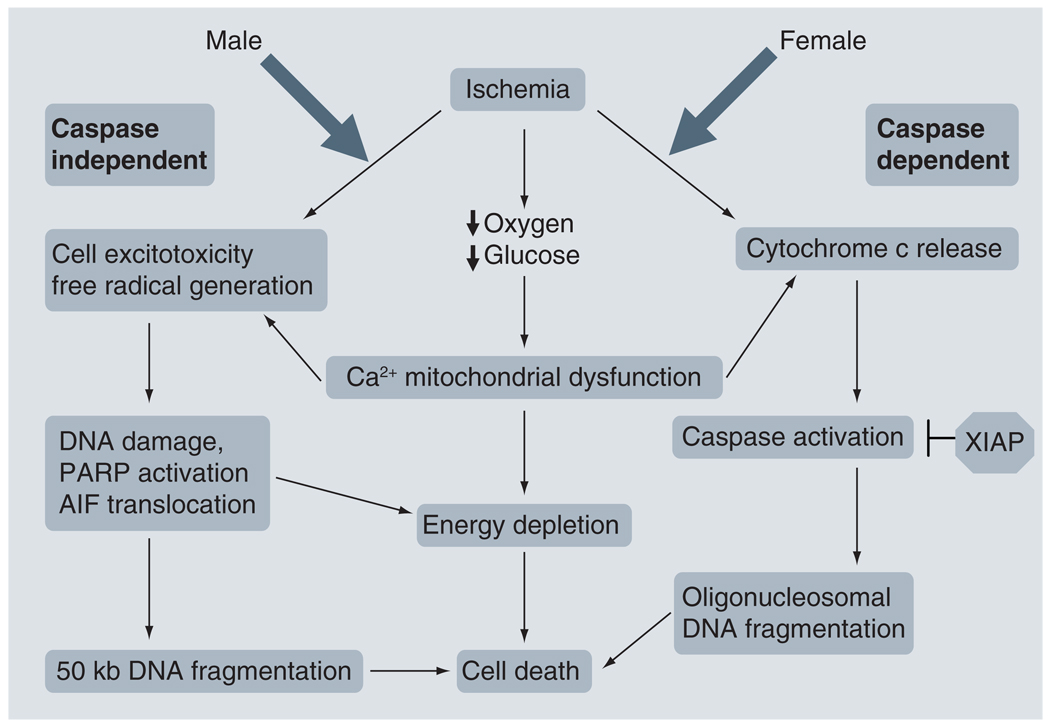
Stroke is a sexually dimorphic disease, with differences between males and females observed both clinically and in the laboratory. While males have a higher incidence of stroke throughout much of the lifespan, aged females have a higher burden of stroke. Sex differences in stroke result from a combination of factors, including elements intrinsic to the sex chromosomes as well as the effects of sex hormone exposure throughout the lifespan. Research investigating the sexual dimorphism of stroke is only in the beginning stages, but early findings suggest that different cell death pathways are activated in males and females after ischemic stroke. A greater understanding of the mechanisms underlying sex differences in stroke will lead to more appropriate treatment strategies for patients of both sexes.
Figures
References
-
- Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics – 2009 update: a report from the American Heart Association statistics committee and stroke statistics subcommittee. Circulation. 2009;119(3):480–486. - PubMed
-
- Rojas JI, Zurru MC, Romano M, Patrucco L, Cristiano E. Acute ischemic stroke and transient ischemic attack in the very old – risk factor profile and stroke subtype between patients older than 80 years and patients aged less than 80 years. Eur. J. Neurol. 2007;14(8):895–899. - PubMed
-
- Kleindorfer D, Broderick J, Khoury J, et al. The unchanging incidence and case-fatality of stroke in the 1990s: a population-based study. Stroke. 2006;37(10):2473–2478. - PubMed
-
- Putaala J, Metso AJ, Metso TM, et al. Analysis of 1008 consecutive patients aged 15 to 49 with first-ever ischemic stroke: the Helsinki young stroke registry. Stroke. 2009;40(4):1195–1203. - PubMed
-
- Armstrong-Wells J, Johnston SC, Wu YW, Sidney S, Fullerton HJ. Prevalence and predictors of perinatal hemorrhagic stroke: results from the Kaiser Pediatric Stroke Study. Pediatrics. 2009;123(3):823–828. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources