

Physiotherapy and low back pain in the injured worker: an examination of current practice during the subacute phase of healing
- PMID: 20190991
- PMCID: PMC2792240
- DOI: 10.3138/physio.61.2.88
Physiotherapy and low back pain in the injured worker: an examination of current practice during the subacute phase of healing
Abstract
Purpose: To describe current physiotherapy practice for injured workers with subacute low back pain (SA-LBP).
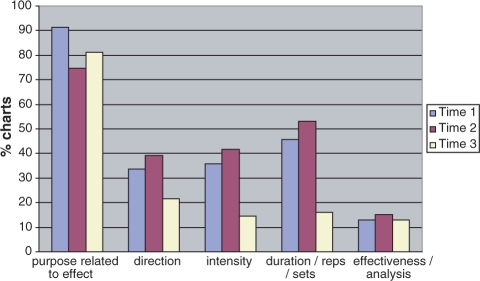
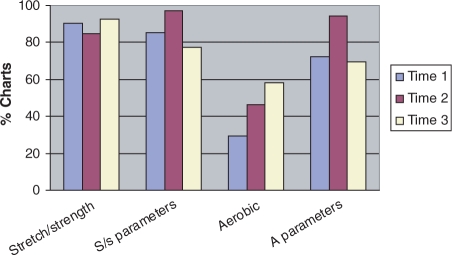
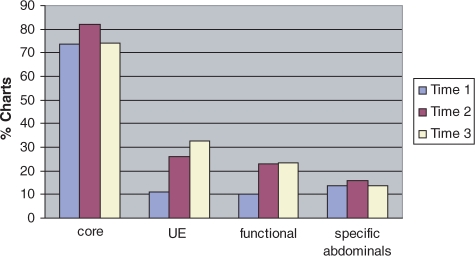
Method: A chart audit of discharged workers was conducted over three episodes of care: 4-6 weeks (T1), 6-8 weeks (T2), and 8-10 weeks (T3) post-injury. The prevalence and reproducibility of parameters for common interventions were calculated as the percentage of active charts over time. Focus groups were used to validate audit results and deepen our understanding of practice.
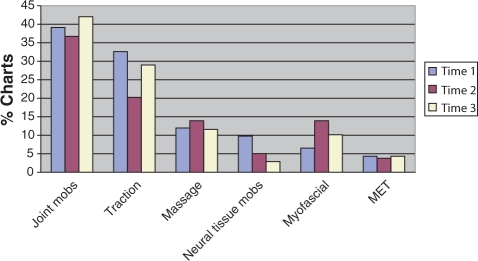
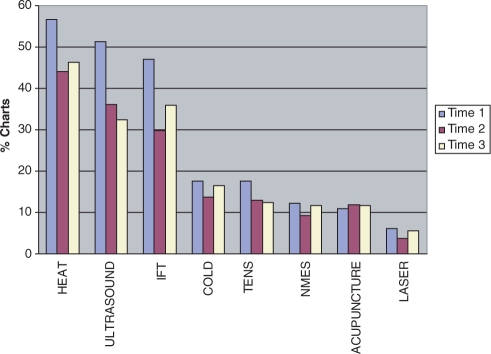
Results: In all, 164 charts were audited. The most prevalent interventions were (1) for manual therapy, joint mobilization and traction; (2) for electrophysical agents (EPAs), heat, ultrasound, and interferential therapy; and (3) for exercise, core stabilization exercises. Transcript analyses revealed that participants viewed injured workers with SA-LBP in a positive light, emphasized the importance of physiotherapy, and discussed SA-LBP in five themes: time frame, non-specific diagnosis, mixed client outlook, change in pain presentation, and the transition from a passive to a more active treatment approach.
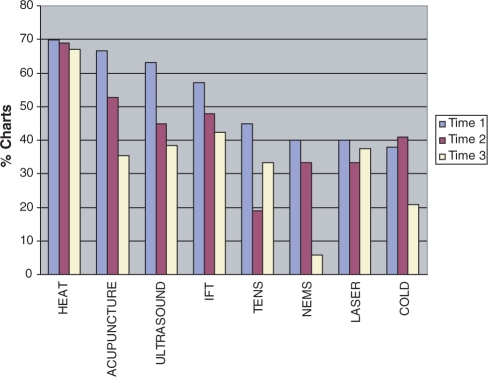
Conclusions: The pattern of decreasing passive and increasing active interventions is consistent with the focus-group participants' description of how they approach treatment of clients with SA-LBP. Also noted was a higher prevalence of interventions poorly supported by evidence and lower prevalence of interventions well supported by evidence.
Objectif : Décrire la pratique actuelle en physiothérapie pour les accidentés du travail atteints d'une lombalgie dans la phase subaiguë de guérison.
Méthode : On a examiné les dossiers de travailleurs ayant reçu leur congé, et ce, en fonction de 3 périodes de traitement : de 4 à 6 (T1), de 6 à 8 (T2) et de 8 à 10 semaines après la survenue de la lésion. La prévalence et la reproductibilité des paramètres inhérents aux interventions courantes ont été calculées par rapport au pourcentage des dossiers actifs au fil du temps. On a fait appel à des groupes de discussion pour valider les résultats de l'examen des dossiers et mieux comprendre la pratique.
Résultats : L'examen a porté sur 164 dossiers. Les modalités d'intervention les plus courantes ont été (1) la mobilisation articulaire et la traction en matière de thérapeutique manuelle ; (2) la chaleur, les ultrasons et l'électrothérapie à courants interférentiels pour ce qui est des agents électrophysiologiques et (3) les exercices de stabilisation des muscles du tronc pour ce qui est des exercices. L'analyse des transcriptions a révélé que les participants avaient une opinion positive des accidentés du travail souffrant de lombalgie subaiguë; ils ont souligné l'importance de la physiothérapie et ont abordé la lombalgie subaiguë en fonction de 5 thèmes : le bloc de temps, le diagnostic non spécifique, le portrait diversifié de la clientèle, le tableau changeant de la douleur et la démarche thérapeutique (transition d'un traitement passif à un traitement plus active au cours de la période du traitement).
Conclusions : La tendance voulant que l'on intervienne de plus en plus activement cadre avec la façon dont les groupes de discussion ont décrit leur démarche thérapeutique auprès des patients souffrant de lombalgie subaiguë. Il est par ailleurs à noter que la prévalence des interventions moins bien étayées était supérieure à celle des interventions recueillant un fort appui.
Keywords: chart audit; electrophysical agents; exercise; focus groups; manual therapy; subacute low back pain.
Figures
Similar articles
-
Client Education: Communicative Interaction between Physiotherapists and Clients with Subacute Low Back Pain in Private Practice.Physiother Can. 2011 Spring;63(2):212-23. doi: 10.3138/ptc.2009-52P. Epub 2011 Apr 13. Physiother Can. 2011. PMID: 22379262 Free PMC article.
-
Physical therapists' treatment choices for non-specific low back pain in Florida: an electronic survey.J Man Manip Ther. 2015 May;23(2):109-18. doi: 10.1179/2042618613Y.0000000065. J Man Manip Ther. 2015. PMID: 26109832 Free PMC article.
-
Management of work-related low back pain: a population-based survey of physical therapists.Phys Ther. 2005 Nov;85(11):1168-81. Phys Ther. 2005. PMID: 16253046
-
[Subgroup-specific therapy of low back pain: description and validity of two classification systems].Orthopade. 2013 Feb;42(2):90-9. doi: 10.1007/s00132-012-2041-5. Orthopade. 2013. PMID: 23370728 Review. German.
-
Therapeutic ultrasound for chronic low back pain.Cochrane Database Syst Rev. 2020 Jul 5;7(7):CD009169. doi: 10.1002/14651858.CD009169.pub3. Cochrane Database Syst Rev. 2020. PMID: 32623724 Free PMC article.
Cited by
-
Clinician's Commentary on Cutforth et al.(1).Physiother Can. 2011 Summer;63(3):287-8. doi: 10.3138/physio.63.3.287. Epub 2011 Aug 10. Physiother Can. 2011. PMID: 22654234 Free PMC article. No abstract available.
-
Therapeutic Effect of Movement Control Exercises Combined With Traditional Physiotherapeutic Rehabilitation in A Patient Suffering With Non-Specific Low Back Pain: A Case Report.Cureus. 2024 Jun 7;16(6):e61868. doi: 10.7759/cureus.61868. eCollection 2024 Jun. Cureus. 2024. PMID: 38978892 Free PMC article.
-
Research designs and instruments to detect physiotherapy overuse of low-value care services in low back pain management: a scoping review.BMC Health Serv Res. 2023 Feb 23;23(1):193. doi: 10.1186/s12913-023-09166-4. BMC Health Serv Res. 2023. PMID: 36823581 Free PMC article.
-
Implementing the work disability prevention paradigm among therapists in Hong Kong: facilitators and barriers.J Occup Rehabil. 2011 Mar;21(1):76-83. doi: 10.1007/s10926-010-9256-2. J Occup Rehabil. 2011. PMID: 20652377
-
Evaluating physical therapy students' knowledge of and adherence to the ambassador low back pain guideline.Physiother Can. 2013 Fall;65(4):384-95. doi: 10.3138/ptc.2012-33. Physiother Can. 2013. PMID: 24396169 Free PMC article.
References
-
- Merskey H, Bogduk N, editors. Classification of chronic pain: descriptions of chronic pain syndrome and definitions of pain terms. 2nd. Seattle, WA: IASP Press; 1994.
-
- Waddell G. The back pain revolution. Toronto: Churchill Livingstone; 1998.
-
- Canadian Pain Society Task Force on Wait Times. Establishing acceptable waiting times for treatment of pain in Canada. Oshawa, ON: Canadian Pain Society; 2006.
-
- Ospina M, Harstall C. Prevalence of chronic pain: an overview. Edmonton: Alberta Heritage Foundation for Medical Research, Health Technology Assessment; 2002.
LinkOut - more resources
Full Text Sources
Miscellaneous