

Fatal biliary-systemic air embolism during endoscopic retrograde cholangiopancreatography: a case with multifocal liver abscesses and choledochoduodenostomy
- PMID: 20191026
- PMCID: PMC2824879
- DOI: 10.3349/ymj.2010.51.2.287
Fatal biliary-systemic air embolism during endoscopic retrograde cholangiopancreatography: a case with multifocal liver abscesses and choledochoduodenostomy
Abstract
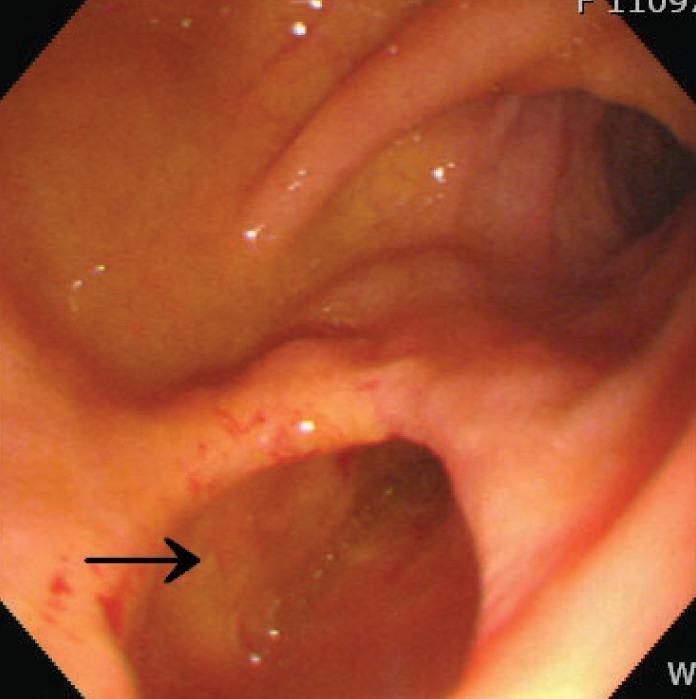
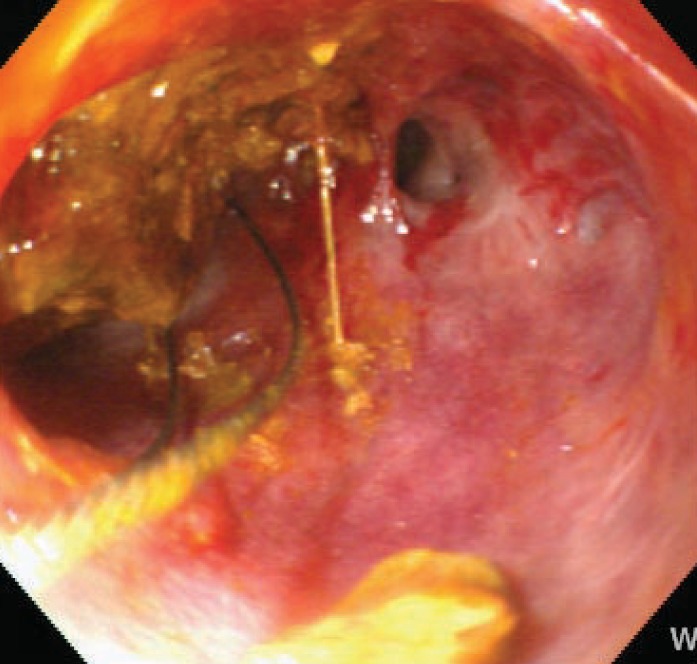
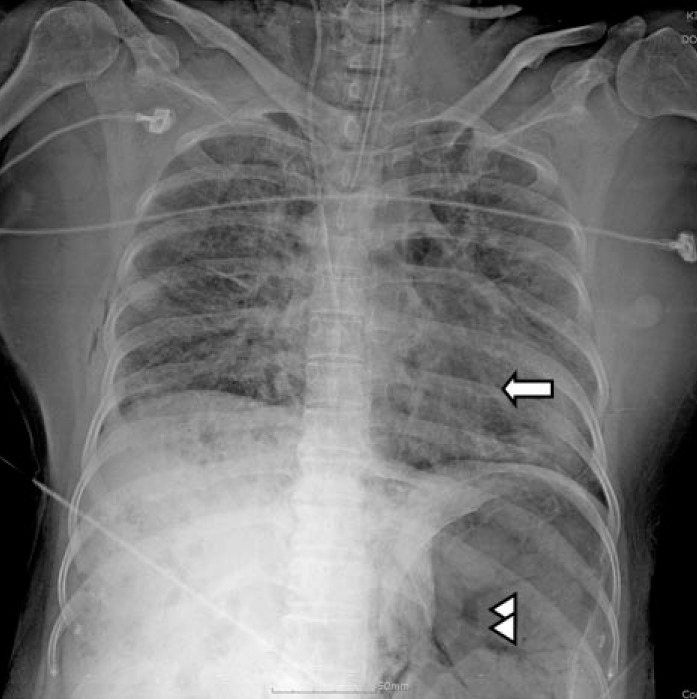
We report a rare case of a massive fatal embolism that occurred in the middle of endoscopic retrograde cholangiopancreatography (ERCP) and retrospectively examine the significant causes of the event. The patient was a 50-year old female with an uncertain history of previous abdominal surgery for multiple biliary stones 20 years prior. The patient presented with acute right upper quadrant pain. An abdominal computed tomographic (CT) scan revealed the presence of multiple stones in the common bile duct (CBD) and intra-hepatic duct (IHD) with biliary obstruction, multifocal liver abscesses, and air-biliarygram. Emergency ERCP showed a wide and straight opening of choledochoduodenostomy, which may have been created during a previous surgery, and multiple filling defects in the CBD. With the use of a forward endoscope, mud stones were extracted through the opening of the choledochoduodenostomy. Cardiac arrest suddenly developed during the procedure, and despite immediate resuscitation, the patient died due to a massive systemic air embolism. We reviewed previously reported fatal cases and accessed factors facilitating air embolisms in this case.
Keywords: Air embolism; ERCP; choledochoduodenostomy; sphincterotomy.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures

Similar articles
-
Fatal systemic venous air embolism during endoscopic retrograde cholangiopancreatography.Adv Anat Pathol. 2009 Jul;16(4):255-62. doi: 10.1097/PAP.0b013e3181aab793. Adv Anat Pathol. 2009. PMID: 19546613
-
[Thoracoabdominal CT scan: a useful tool for the diagnosis of air embolism during an endoscopic retrograde cholangiopancreatography].Ann Fr Anesth Reanim. 2008 Mar;27(3):240-3. doi: 10.1016/j.annfar.2007.12.015. Epub 2008 Mar 4. Ann Fr Anesth Reanim. 2008. PMID: 18313255 French.
-
Laparoscopic choledochoduodenostomy.Surg Laparosc Endosc. 1996 Aug;6(4):318-21. Surg Laparosc Endosc. 1996. PMID: 8840458
-
Obstructive jaundice due to a blood clot after ERCP: a case report and review of the literature.BMC Gastroenterol. 2018 Nov 3;18(1):163. doi: 10.1186/s12876-018-0898-4. BMC Gastroenterol. 2018. PMID: 30390657 Free PMC article. Review.
-
Endoscopic ultrasonographic access and drainage of the common bile duct.Gastrointest Endosc Clin N Am. 2013 Apr;23(2):435-52. doi: 10.1016/j.giec.2012.12.013. Epub 2013 Jan 30. Gastrointest Endosc Clin N Am. 2013. PMID: 23540968 Review.
Cited by
-
Gas embolism during endoscopic retrograde cholangiopancreatography: diagnosis and management.Ann Gastroenterol. 2019 Mar-Apr;32(2):156-167. doi: 10.20524/aog.2018.0339. Epub 2018 Dec 20. Ann Gastroenterol. 2019. PMID: 30837788 Free PMC article. Review.
-
Air embolism complicating gastrointestinal endoscopy: A systematic review.World J Gastrointest Endosc. 2013 Aug 16;5(8):359-65. doi: 10.4253/wjge.v5.i8.359. World J Gastrointest Endosc. 2013. PMID: 23951390 Free PMC article.
-
When in Trouble Think of the Bubble: Paradoxical Cerebral Arterial Gas Embolism after Endoscopic Retrograde Cholangiopancreatography.Case Rep Gastroenterol. 2021 Apr 29;15(1):456-469. doi: 10.1159/000514706. eCollection 2021 Jan-Apr. Case Rep Gastroenterol. 2021. PMID: 34054400 Free PMC article.
-
Capnography in the endoscopy suite: A necessity, not a luxury!Indian J Anaesth. 2017 Aug;61(8):689-690. doi: 10.4103/ija.IJA_406_17. Indian J Anaesth. 2017. PMID: 28890572 Free PMC article. No abstract available.
-
Clinical Presentation, Diagnosis, and Management of Air Embolism During Endoscopic Retrograde Cholangiopancreatography.Gastroenterology Res. 2019 Dec;12(6):283-287. doi: 10.14740/gr1208. Epub 2019 Nov 21. Gastroenterology Res. 2019. PMID: 31803307 Free PMC article. Review.
References
-
- Nayagam J, Ho KM, Liang J. Fatal systemic air embolism during endoscopic retrograde cholangio-pancreatography. Anaesth Intensive Care. 2004;32:260–264. - PubMed
-
- Christi SU, Scheppach W, Peters U, Kirchner T. Cerebral air embolism after gastroduodenoscopy: complication of a duodenocaval fistula. Gastrointest Endosc. 1994;40:376–378. - PubMed
-
- Raju GS, Bcndixen BH, Khan J, Summers RW. Cerebrovascular accident during endoscopy: consider cerebral air embolism, a rapidly reversible event with hyperbaric oxygen therapy. Gastrointest Endosc. 1998;47:70–73. - PubMed
-
- Akhtar N, Jafri W, Mozaffar T. Cerebral artery air embolism following an esophagogastroscopy: a case report. Neurology. 2001;56:136–137. - PubMed
-
- Kennedy C, Larvin M, Linsell J. Fatal hepatic air embolism following ERCR. Gastrointest Endosc. 1997;45:187–188. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
