

Prophylaxis of chemotherapy-induced febrile neutropenia with granulocyte colony-stimulating factors: where are we now?
- PMID: 20191292
- PMCID: PMC2846279
- DOI: 10.1007/s00520-010-0816-y
Prophylaxis of chemotherapy-induced febrile neutropenia with granulocyte colony-stimulating factors: where are we now?
Abstract
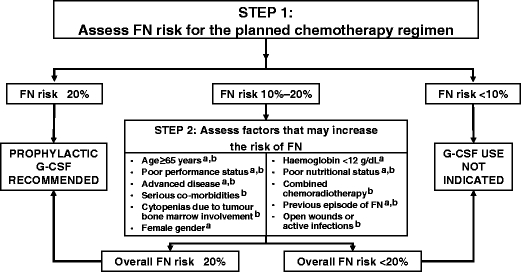
Updated international guidelines published in 2006 have broadened the scope for the use of granulocyte colony-stimulating factor (G-CSF) in supporting delivery of myelosuppressive chemotherapy. G-CSF prophylaxis is now recommended when the overall risk of febrile neutropenia (FN) due to regimen and individual patient factors is >or=20%, for supporting dose-dense and dose-intense chemotherapy and to help maintain dose density where dose reductions have been shown to compromise outcomes. Indeed, there is now a large body of evidence for the efficacy of G-CSFs in supporting dose-dense chemotherapy. Predictive tools that can help target those patients who are most at risk of FN are now becoming available. Recent analyses have shown that, by reducing the risk of FN and chemotherapy dose delays and reductions, G-CSF prophylaxis can potentially enhance survival benefits in patients receiving chemotherapy in curative settings. Accumulating data from 'real-world' clinical practice settings indicate that patients often receive abbreviated courses of daily G-CSF and consequently obtain a reduced level of FN protection. A single dose of PEGylated G-CSF (pegfilgrastim) may provide a more effective, as well as a more convenient, alternative to daily G-CSF. Prospective studies are needed to validate the importance of delivering the full dose intensity of standard chemotherapy regimens, with G-CSF support where appropriate, across a range of settings. These studies should also incorporate prospective evaluation of risk stratification for neutropenia and its complications.
Figures
References
-
- Caggiano V, Weiss RV, Rickert TS, Linde-Zwirble WT. Incidence, cost, and mortality of neutropenia hospitalization associated with chemotherapy. Cancer. 2005;103:1916–1924. - PubMed
-
- Courtney DM, Aldeen AZ, Gorman SM, Handler JA, Trifilio SM, Parada JP, Yarnold PR, Bennett CL. Cancer-associated neutropenic fever: clinical outcome and economic costs of emergency department care. Oncologist. 2007;12:1019–1026. - PubMed
-
- Kuderer NM, Dale DC, Crawford J, Cosler LE, Lyman GH. Mortality, morbidity, and cost associated with febrile neutropenia in adult cancer patients. Cancer. 2006;106:2258–2266. - PubMed
-
- Mayordomo JI, Castellanos J, Pernas S, Ruiz-Borrego M, Velasco A, Frau A, Lamas MJ, Lara N, Gasquet JA, Sánchez J. Cost analysis of febrile neutropenia management of breast cancer patients in clinical practice in Spain. Ann Oncol. 2006;17(Suppl 9):ix190–ix195.
-
- Elting LS, Lu C, Escalante CP, Giordano SH, Trent JC, Cooksley C, Avritscher EB, Shih YC, Ensor J, Bekele BN, Gralla RJ, Talcott JA, Rolston K. Outcomes and cost of outpatient or inpatient management of 712 patients with febrile neutropenia. J Clin Oncol. 2008;26:606–611. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
