

Physician preference motivates the use of anti-tumor necrosis factor therapy independent of clinical disease activity
- PMID: 20191497
- PMCID: PMC2913388
- DOI: 10.1002/acr.20020
Physician preference motivates the use of anti-tumor necrosis factor therapy independent of clinical disease activity
Abstract
Objective: Physician preference has previously been shown to be an important determinant of prescription patterns, independent of patient-specific factors. We evaluated whether physician preference was important in the decision to select anti-tumor necrosis factor (anti-TNF) therapy rather than nonbiologic disease-modifying antirheumatic drugs (DMARDs) among rheumatoid arthritis (RA) patients initiating a new RA medication.
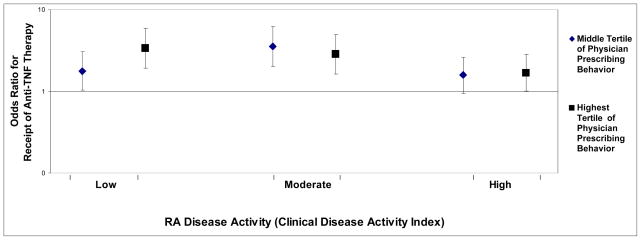
Methods: Using data from the Consortium of Rheumatology Researchers of North America, we identified RA patients who had never taken biologics initiating either anti-TNF therapy or a DMARD in 2001-2008. Physician preference for the use of anti-TNF agents was calculated using data from the preceding calendar year for each physician's other RA patients. Multivariable logistic regression with generalized estimating equations accounted for clustering of patients within the physician practice and evaluated the relationship between physician preference and receipt of anti-TNF therapy, controlling for patient-related factors and disease activity using the Clinical Disease Activity Index.
Results: We identified 1,532 RA patients initiating anti-TNF therapy or a DMARD. In models adjusting for tender and swollen joint counts and global disease activity, physician preference for the use of anti-TNF therapy was an independent predictor of receipt of these agents. Patients of physicians in the highest and middle tertiles of physician preference had a 2.50 (95% confidence interval [95% CI] 1.76-3.56) and 1.70 (95% CI 1.22-2.39) greater likelihood of receiving anti-TNF medications, respectively.
Conclusion: Physician preference is an important determinant of patients' receipt of anti-TNF therapy and may be useful to examine in future studies of RA treatment patterns, costs, and medication safety.
Figures
Comment in
-
Physician preference: filling the evidence gap.Arthritis Care Res (Hoboken). 2010 Jan 15;62(1):1-3. doi: 10.1002/acr.20006. Arthritis Care Res (Hoboken). 2010. PMID: 20191484 No abstract available.
References
-
- Schneeweiss S, Glynn RJ, Avorn J, Solomon DH. A Medicare database review found that physician preferences increasingly outweighed patient characteristics as determinants of first-time prescriptions for COX-2 inhibitors. J Clin Epidemiol. 2005 Jan;58(1):98–102. - PubMed
-
- Solomon DH, Schneeweiss S, Glynn RJ, Levin R, Avorn J. Determinants of selective cyclooxygenase-2 inhibitor prescribing: are patient or physician characteristics more important? Am J Med. 2003 Dec 15;115(9):715–20. - PubMed
-
- Schneeweiss S, Solomon DH, Wang PS, Rassen J, Brookhart MA. Simultaneous assessment of short-term gastrointestinal benefits and cardiovascular risks of selective cyclooxygenase 2 inhibitors and nonselective nonsteroidal antiinflammatory drugs: an instrumental variable analysis. Arthritis Rheum. 2006 Nov;54(11):3390–8. - PubMed
-
- Greenland S. An introduction to instrumental variables for epidemiologists. Int J Epidemiol. 2000 Aug;29(4):722–9. - PubMed
-
- Kremer JM. The CORRONA database. Autoimmun Rev. 2006 Jan;5(1):46–54. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
