

Cost-effectiveness of preparticipation screening for prevention of sudden cardiac death in young athletes
- PMID: 20194233
- PMCID: PMC2873148
- DOI: 10.7326/0003-4819-152-5-201003020-00005
Cost-effectiveness of preparticipation screening for prevention of sudden cardiac death in young athletes
Abstract
Background: Inclusion of 12-lead electrocardiography (ECG) in preparticipation screening of young athletes is controversial because of concerns about cost-effectiveness.
Objective: To evaluate the cost-effectiveness of ECG plus cardiovascular-focused history and physical examination compared with cardiovascular-focused history and physical examination alone for preparticipation screening.
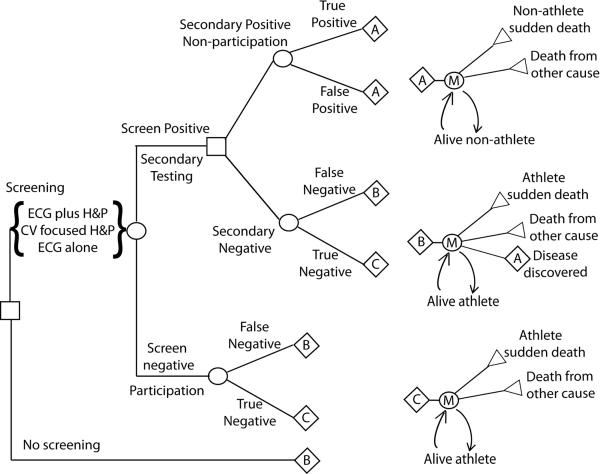
Design: Decision-analysis, cost-effectiveness model.
Data sources: Published epidemiologic and preparticipation screening data, vital statistics, and other publicly available data.
Target population: Competitive athletes in high school and college aged 14 to 22 years.
Time horizon: Lifetime.
Perspective: Societal.
Intervention: Nonparticipation in competitive athletic activity and disease-specific treatment for identified athletes with heart disease.
Outcome measure: Incremental health care cost per life-year gained.
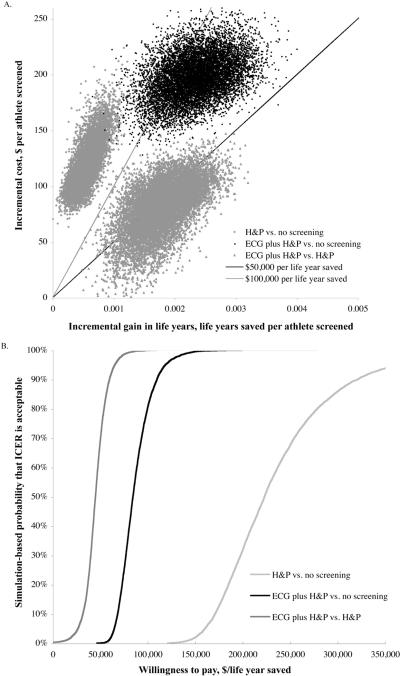
Results of base-case analysis: Addition of ECG to preparticipation screening saves 2.06 life-years per 1000 athletes at an incremental total cost of $89 per athlete and yields a cost-effectiveness ratio of $42 900 per life-year saved (95% CI, $21 200 to $71 300 per life-year saved) compared with cardiovascular-focused history and physical examination alone. Compared with no screening, ECG plus cardiovascular-focused history and physical examination saves 2.6 life-years per 1000 athletes screened and costs $199 per athlete, yielding a cost-effectiveness ratio of $76 100 per life-year saved ($62 400 to $130 000).
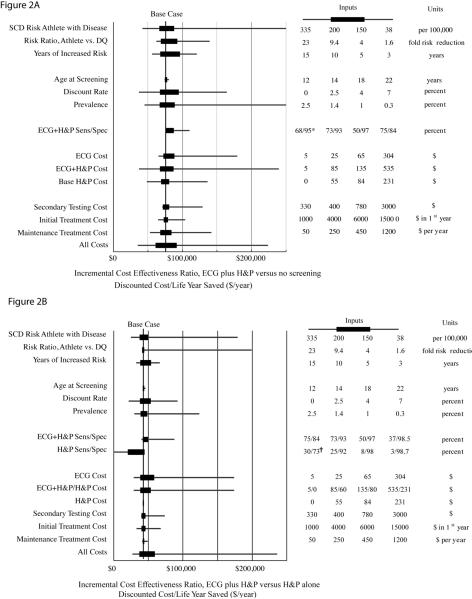
Results of sensitivity analysis: Results are sensitive to the relative risk reduction associated with nonparticipation and the cost of initial screening.
Limitations: Effectiveness data are derived from 1 major European study. Patterns of causes of sudden death may vary among countries.
Conclusion: Screening young athletes with 12-lead ECG plus cardiovascular-focused history and physical examination may be cost-effective.
Primary funding source: Stanford Cardiovascular Institute and the Breetwor Foundation.
Figures
Comment in
-
Summaries for patients. Cost-effectiveness of different types of evaluations before sports participation in young athletes.Ann Intern Med. 2010 Mar 2;152(5):I40. doi: 10.7326/0003-4819-152-5-201003020-00002. Ann Intern Med. 2010. PMID: 20194229 No abstract available.
-
National electrocardiography screening for competitive athletes: Feasible in the United States?Ann Intern Med. 2010 Mar 2;152(5):324-6. doi: 10.7326/0003-4819-152-5-201003020-00012. Ann Intern Med. 2010. PMID: 20194239 No abstract available.
-
Prevention: Potential benefits of ECG screening in young athletes.Nat Rev Cardiol. 2010 May;7(5):240. doi: 10.1038/nrcardio.2010.47. Nat Rev Cardiol. 2010. PMID: 20425901 No abstract available.
-
Should electrocardiography be used in cardiovascular screening of high school athletes?Ann Intern Med. 2010 Jul 6;153(1):64; author reply 64-5. doi: 10.7326/0003-4819-153-1-201007060-00027. Ann Intern Med. 2010. PMID: 20621918 No abstract available.
References
-
- Maron BJ. Hypertrophic cardiomyopathy and other causes of sudden cardiac death in young competitive athletes, with considerations for preparticipation screening and criteria for disqualification. Cardiol Clin. 2007;25(3):399–414. - PubMed
-
- Drezner JA, Chun JSDY, Harmon KG, Derminer L. Survival trends in the United States following exercise-related sudden cardiac arrest in the youth: 2000–2006. Heart Rhythm. 2008;5(6):794–799. - PubMed
-
- Corrado D, Basso C, Rizzoli G, Schiavon M, Thiene G. Does sports activity enhance the risk of sudden death in adolescents and young adults? J Am Coll Cardiol. 2003;42(11):1959–63. - PubMed
-
- Thompson PD, Franklin BA, Balady GJ, Blair SN, Corrado D, Estes NA, 3rd, et al. Exercise and acute cardiovascular events placing the risks into perspective: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism and the Council on Clinical Cardiology. Circulation. 2007;115(17):2358–68. - PubMed
-
- Van Camp SP, Bloor CM, Mueller FO, Cantu RC, Olson HG. Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc. 1995;27(5):641–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials