

Systematic review: Vitamin D and cardiometabolic outcomes
- PMID: 20194237
- PMCID: PMC3211092
- DOI: 10.7326/0003-4819-152-5-201003020-00009
Systematic review: Vitamin D and cardiometabolic outcomes
Abstract
Background: Vitamin D may modify risk for cardiometabolic outcomes (type 2 diabetes, hypertension, or cardiovascular disease).
Purpose: To examine the association between vitamin D status, including the effect of vitamin D supplementation, and cardiometabolic outcomes in generally healthy adults.
Data sources: English-language studies in MEDLINE (inception to 4 November 2009) and the Cochrane Central Register of Controlled Trials (fourth quarter of 2009).
Study selection: 11 reviewers screened citations to identify longitudinal cohort studies that reported associations between vitamin D status and cardiometabolic outcomes, including randomized trials of vitamin D supplementation.
Data extraction: 5 independent reviewers extracted data about study conduct, participant characteristics, outcomes, and quality. Differences were resolved by consensus.
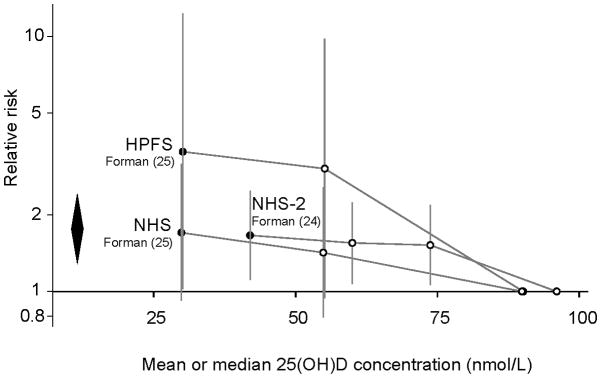
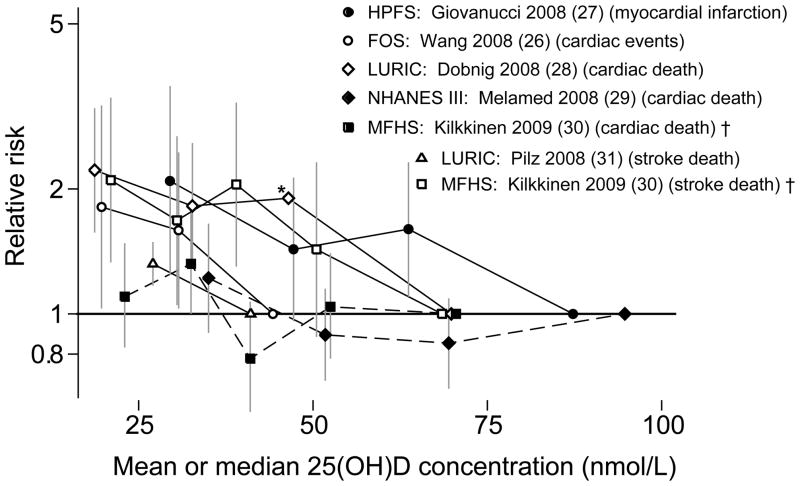
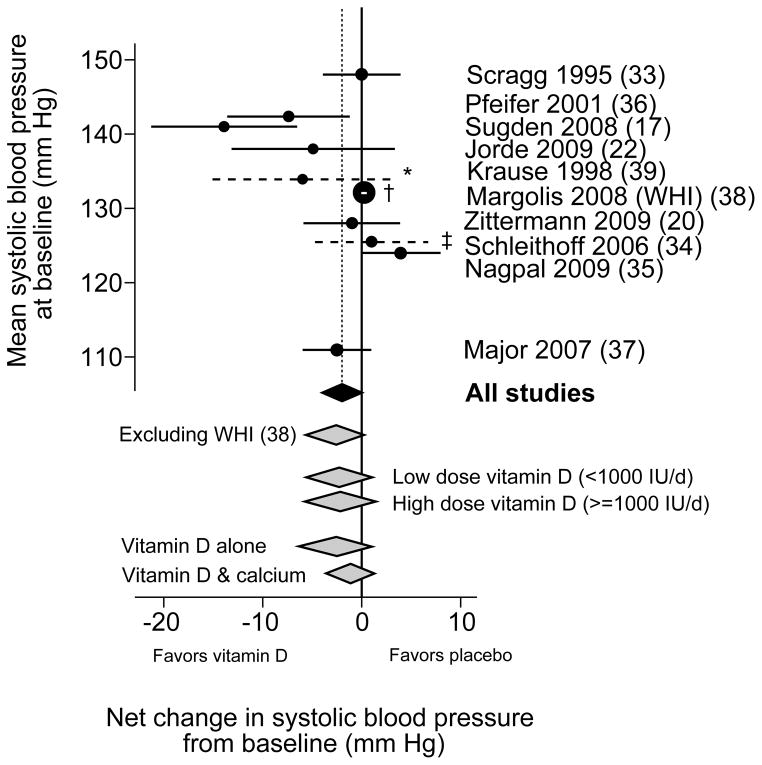
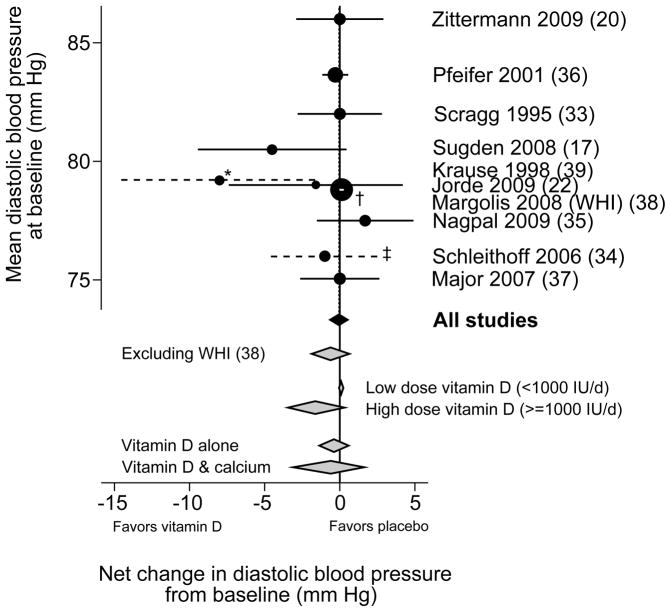
Data synthesis: 13 observational studies (14 cohorts) and 18 trials were eligible. Three of 6 analyses (from 4 different cohorts) reported a lower incident diabetes risk in the highest versus the lowest vitamin D status groups. Eight trials found no effect of vitamin D supplementation on glycemia or incident diabetes. In meta-analysis of 3 cohorts, lower 25-hydroxyvitamin D concentration was associated with incident hypertension (relative risk, 1.8 [95% CI, 1.3 to 2.4]). In meta-analyses of 10 trials, supplementation nonsignificantly reduced systolic blood pressure (weighted mean difference, -1.9 mm Hg [CI, -4.2 to 0.4 mm Hg]) and did not affect diastolic blood pressure (weighted mean difference, -0.1 mm Hg [CI, -0.7 to 0.5 mm Hg]). Lower 25-hydroxyvitamin D concentration was associated with incident cardiovascular disease in 5 of 7 analyses (6 cohorts). Four trials found no effect of supplementation on cardiovascular outcomes.
Limitations: Studies included primarily white participants. Observational studies were heterogeneous. Several trials reported post hoc analyses.
Conclusion: The association between vitamin D status and cardiometabolic outcomes is uncertain. Trials showed no clinically significant effect of vitamin D supplementation at the dosages given.
Primary funding source: National Institute of Diabetes and Digestive and Kidney Disease, the National Institutes of Health Office of Dietary Supplements, U.S. Food and Drug Administration, Agency for Healthcare Research and Quality, and Public Health Agency of Canada.
Conflict of interest statement
Potential Financial Conflicts of Interest: None disclosed.
Figures
Comment in
-
Vitamin D supplementation in the age of lost innocence.Ann Intern Med. 2010 Mar 2;152(5):327-9. doi: 10.7326/0003-4819-152-5-201003020-00013. Ann Intern Med. 2010. PMID: 20194240 No abstract available.
-
Does inconclusive evidence for vitamin D supplementation to reduce risk for cardiovascular disease warrant pessimism?Ann Intern Med. 2010 Aug 3;153(3):208-9; author reply 209-10. doi: 10.7326/0003-4819-153-3-201008030-00016. Ann Intern Med. 2010. PMID: 20679567 No abstract available.
-
Does inconclusive evidence for vitamin D supplementation to reduce risk for cardiovascular disease warrant pessimism?Ann Intern Med. 2010 Aug 3;153(3):208; author reply 209-10. doi: 10.7326/0003-4819-153-3-201008030-00015. Ann Intern Med. 2010. PMID: 20679568 No abstract available.
-
Does inconclusive evidence for vitamin D supplementation to reduce risk for cardiovascular disease warrant pessimism?Ann Intern Med. 2010 Aug 3;153(3):209; author reply 209-10. doi: 10.7326/0003-4819-153-3-201008030-00017. Ann Intern Med. 2010. PMID: 20679570 No abstract available.
References
-
- Kendrick J, Targher G, Smits G, Chonchol M. 25-Hydroxyvitamin D deficiency is independently associated with cardiovascular disease in the Third National Health and Nutrition Examination Survey. Atherosclerosis. 2008;205(1):255–60. - PubMed
-
- Fleck A. Latitude and ischaemic heart disease. Lancet. 1989;1(8638):613. - PubMed
-
- Rostand SG. Ultraviolet light may contribute to geographic and racial blood pressure differences. Hypertension. 1997;30(2 Pt 1):150–6. - PubMed
-
- Voors AW, Johnson WD. Altitude and arteriosclerotic heart disease mortality in white residents of 99 of the 100 largest cities in the United States. J Chronic Dis. 1979;32(1–2):157–62. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical