

An optimized pentaplex PCR for detecting DNA mismatch repair-deficient colorectal cancers
- PMID: 20195377
- PMCID: PMC2827558
- DOI: 10.1371/journal.pone.0009393
An optimized pentaplex PCR for detecting DNA mismatch repair-deficient colorectal cancers
Erratum in
- PLoS One. 2010;5(3). doi: 10.1371/annotation/572bb6d3-0315-40b1-a6d7-ce818809b5ea doi: 10.1371/annotation/572bb6d3-0315-40b1-a6d7-ce818809b5ea
Abstract
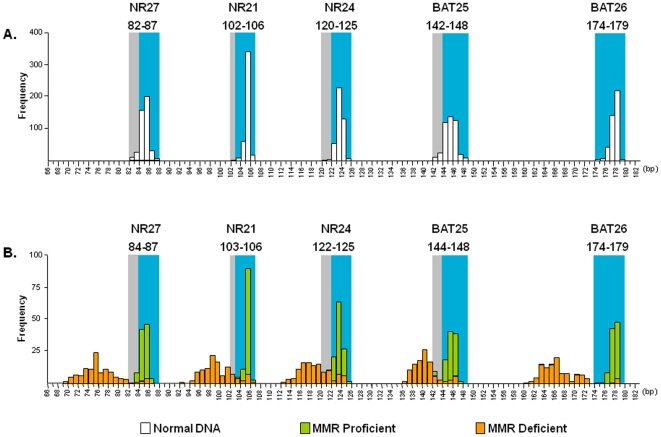
Purpose: Microsatellite instability (MSI) is used to screen colorectal cancers (CRC) for Lynch Syndrome, and to predict outcome and response to treatment. The current technique for measuring MSI requires DNA from normal and neoplastic tissues, and fails to identify tumors with specific DNA mismatch repair (MMR) defects. We tested a panel of five quasi-monomorphic mononucleotide repeat markers amplified in a single multiplex PCR reaction (pentaplex PCR) to detect MSI.
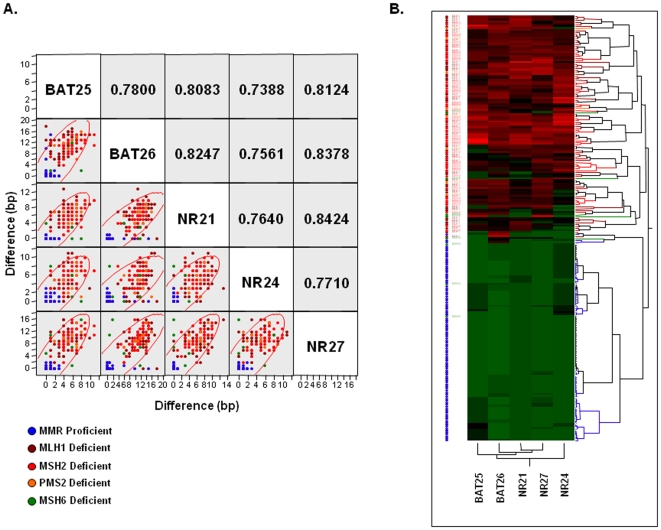
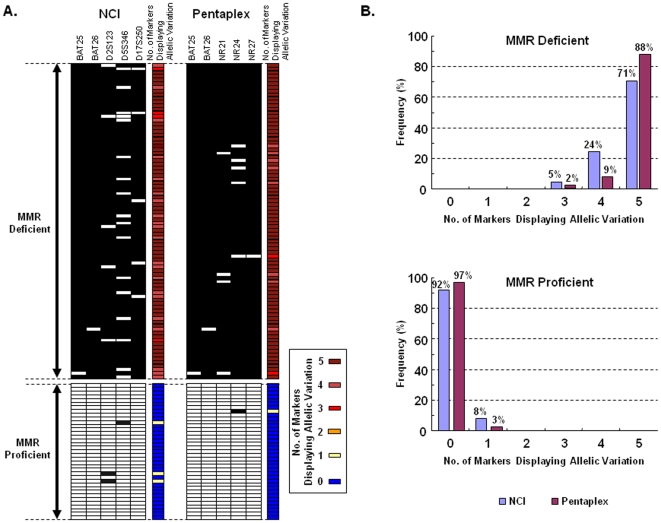
Experimental design: We investigated a cohort of 213 CRC patients, comprised of 114 MMR-deficient and 99 MMR-proficient tumors. Immunohistochemical (IHC) analysis evaluated the expression of MLH1, MSH2, PMS2 and MSH6. MSI status was defined by differences in the quasi-monomorphic variation range (QMVR) from a pool of normal DNA samples, and measuring differences in allele lengths in tumor DNA.
Results: Amplification of 426 normal alleles allowed optimization of the QMVR at each marker, and eliminated the requirement for matched reference DNA to define MSI in each sample. Using > or = 2/5 unstable markers as the criteria for MSI resulted in a sensitivity of 95.6% (95% CI = 90.1-98.1%) and a positive predictive value of 100% (95% CI = 96.6%-100%). Detection of MSH6-deficiency was limited using all techniques. Data analysis with a three-marker panel (BAT26, NR21 and NR27) was comparable in sensitivity (97.4%) and positive predictive value (96.5%) to the five marker panel. Both approaches were superior to the standard approach to measuring MSI.
Conclusions: An optimized pentaplex (or triplex) PCR offers a facile, robust, very inexpensive, highly sensitive, and specific assay for the identification of MSI in CRC.
Conflict of interest statement
Figures

References
-
- Bronner CE, Baker SM, Morrison PT, Warren G, Smith LG, et al. Mutation in the DNA mismatch repair gene homologue hMLH1 is associated with hereditary non-polyposis colon cancer. Nature. 1994;368:258–261. - PubMed
-
- Ionov Y, Peinado MA, Malkhosyan S, Shibata D, Perucho M. Ubiquitous somatic mutations in simple repeated sequences reveal a new mechanism for colonic carcinogenesis. Nature. 1993;363:558–561. - PubMed
-
- Thibodeau SN, Bren G, Schaid D. Microsatellite instability in cancer of the proximal colon. Science. 1993;260:816–819. - PubMed
-
- Kane MF, Loda M, Gaida GM, Lipman J, Mishra R, et al. Methylation of the hMLH1 promoter correlates with lack of expression of hMLH1 in sporadic colon tumors and mismatch repair-defective human tumor cell lines. Cancer Res. 1997;57:808–811. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
