

Biomechanical advantages of dual over single iliac screws in lumbo-iliac fixation construct
- PMID: 20195650
- PMCID: PMC2900011
- DOI: 10.1007/s00586-010-1343-8
Biomechanical advantages of dual over single iliac screws in lumbo-iliac fixation construct
Abstract
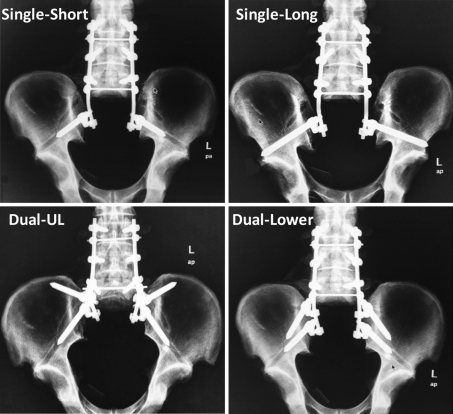
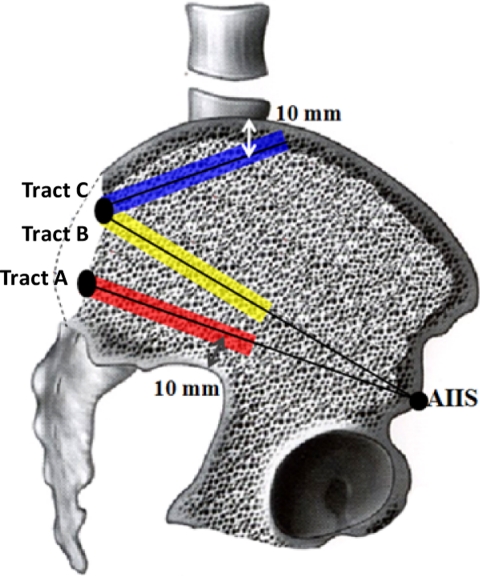
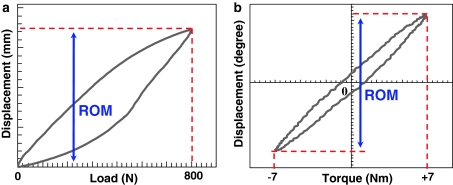
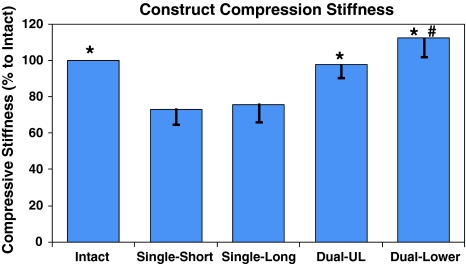
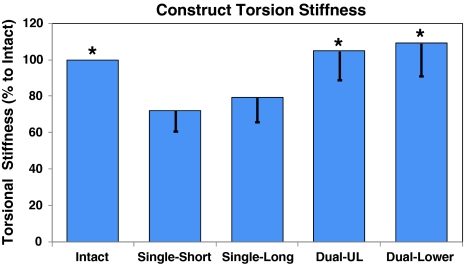
The development of iliac screws has provided a markedly easier way for spino-pelvic instrumentation than the classical Galveston technique. However, high rates of iliac screw loosening and breakage are usually reported, especially in cases where bilateral single iliac screws are used. Therefore, there is a need for exploring more stable iliac fixation techniques. Thus, the objective of this study was to compare the biomechanical effects of bilateral single and dual iliac screws on the stability of L3-iliac fixation construct under total sacrectomy condition. In this study, L2-pelvic specimens were harvested from seven fresh human cadavers. After biomechanically testing the intact state simulated by L3-L5 pedicle screw fixation, destabilization was introduced by total sacrectomy. Upon destabilization, L3-iliac screw-rod reconstructions were performed by four different techniques as follows: (1) bilateral single short iliac screws (Single-Short); (2) bilateral single long iliac screws (Single-Long); (3) bilateral dual short iliac screws, placed in the upper and lower iliac columns (Dual-UL); and (4) bilateral dual short iliac screws, all placed in the lower iliac column (Dual-Lower). These four iliac screw fixation techniques were sequentially preformed in the same specimen, and the lengths of the short and long iliac screws were 70 and 130 mm, respectively. Biomechanical testing was performed on a material testing machine under 800 N compression and 7 Nm torsion loading modes to evaluate the construct stiffness. In compression, the stiffness of the L3-iliac fixation constructs of Single-Short, Single-Long, Dual-UL, and Dual-Lower techniques were 73, 76, 98, and 108% of the intact state, respectively. No significant differences were detected between Single-Short and Single-Long (P = 0.589) techniques. However, the compressive stiffness of these two techniques was significantly lower than the intact state, and the Dual-UL and Dual-Lower techniques (P < 0.05). There was no statistical difference between the intact condition and the Dual-Lower technique (P = 0.109). Interestingly, Dual-Lower exhibited notably higher compressive stiffness than Dual-UL (+10.3%, P = 0.049). In torsion, the stiffness of Single-Short, Single-Long, Dual-UL, and Dual-Lower techniques were 72, 79, 105, and 109% of the intact condition, respectively. No significant differences were detected between Single-Short and Single-Long techniques (P = 0.338), and also among Dual-UL, Dual-lower techniques, and the intact state (P > 0.05). However, Single-Short and Single-Long techniques provided markedly lower construct torsional stiffness than the other three groups (P < 0.05). For lumbo-illiac reconstruction after total sacrectomy, even the use of bilateral single, long iliac screws do not help in restoring the local stability to the intact condition. However, dual iliac screws provide much higher construct stability than single iliac screw techniques. Therefore, dual iliac screw technique should be preferred for treating the unstable situation caused by total sacrectomy.
Figures

Similar articles
-
[Biomechanical effects of iliac screw plates on stability of lumbo-iliac fixation construct].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013 May;27(5):606-11. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013. PMID: 23879102 Chinese.
-
Effect of iliac screw insertion depth on the stability and strength of lumbo-iliac fixation constructs: an anatomical and biomechanical study.Spine (Phila Pa 1976). 2009 Jul 15;34(16):E565-72. doi: 10.1097/BRS.0b013e3181ac8fc4. Spine (Phila Pa 1976). 2009. PMID: 19770599
-
[Biomechanical effect of the iliac screw insertion depth on lumbo-iliac fixation construct].Zhonghua Wai Ke Za Zhi. 2008 Aug 1;46(15):1179-82. Zhonghua Wai Ke Za Zhi. 2008. PMID: 19094686 Chinese.
-
Dual iliac screws in spinopelvic fixation: a systematic review.Eur Spine J. 2019 Sep;28(9):2053-2059. doi: 10.1007/s00586-019-06065-3. Epub 2019 Jul 12. Eur Spine J. 2019. PMID: 31300882
-
[Development and current situation of reconstruction methods following total sacrectomy].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018 May 15;32(5):513-518. doi: 10.7507/1002-1892.201712054. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018. PMID: 29806335 Free PMC article. Review. Chinese.
Cited by
-
Biomechanical evaluation of seven fixation methods to treat pubic symphysis diastasis using finite element analysis.J Orthop Surg Res. 2022 Mar 28;17(1):189. doi: 10.1186/s13018-022-03078-5. J Orthop Surg Res. 2022. PMID: 35346277 Free PMC article.
-
Entry zone of iliac screw fixation to maintain proper entry width and screw length.Eur Spine J. 2015 Nov;24(11):2573-9. doi: 10.1007/s00586-015-4042-7. Epub 2015 May 23. Eur Spine J. 2015. PMID: 26002356
-
Biomechanical tests and finite element analyses of pelvic stability using bilateral single iliac screws with different channels in lumbo-iliac fixation.Front Surg. 2022 Nov 8;9:1035614. doi: 10.3389/fsurg.2022.1035614. eCollection 2022. Front Surg. 2022. PMID: 36425884 Free PMC article.
-
Biomechanical Analysis of the Tuning Fork Plate Versus Dual Pelvic Screws in a Sacrectomy Model: A Finite Element Study.Global Spine J. 2022 Sep;12(7):1495-1502. doi: 10.1177/2192568220983792. Epub 2021 Feb 1. Global Spine J. 2022. PMID: 33517788 Free PMC article.
-
Modified surgical treatment for a patient with neurofibromatosis scoliosis: A case report.World J Orthop. 2020 Nov 18;11(11):523-527. doi: 10.5312/wjo.v11.i11.523. eCollection 2020 Nov 18. World J Orthop. 2020. PMID: 33269219 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
