

Phase I combination of sorafenib and erlotinib therapy in solid tumors: safety, pharmacokinetic, and pharmacodynamic evaluation from an expansion cohort
- PMID: 20197396
- PMCID: PMC2838726
- DOI: 10.1158/1535-7163.MCT-09-0868
Phase I combination of sorafenib and erlotinib therapy in solid tumors: safety, pharmacokinetic, and pharmacodynamic evaluation from an expansion cohort
Abstract
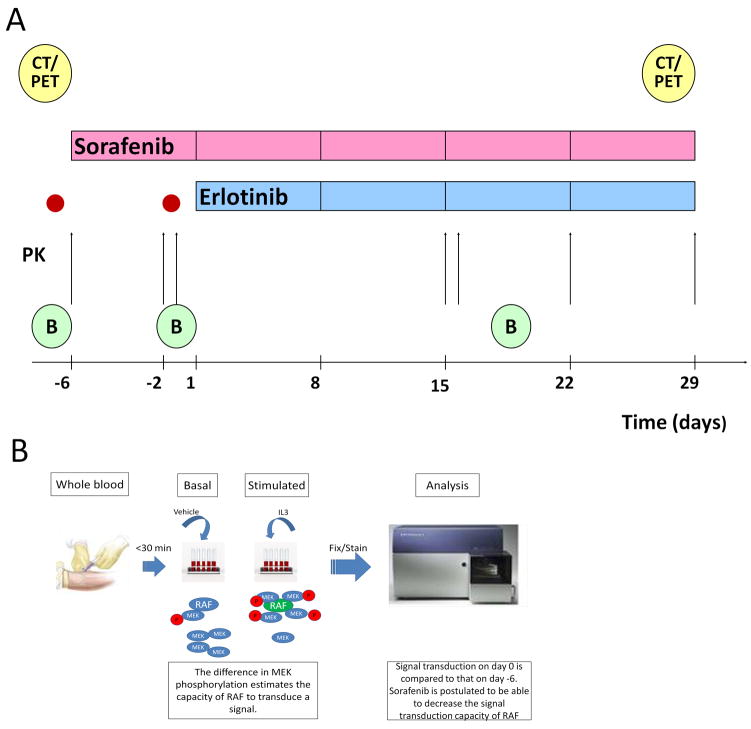
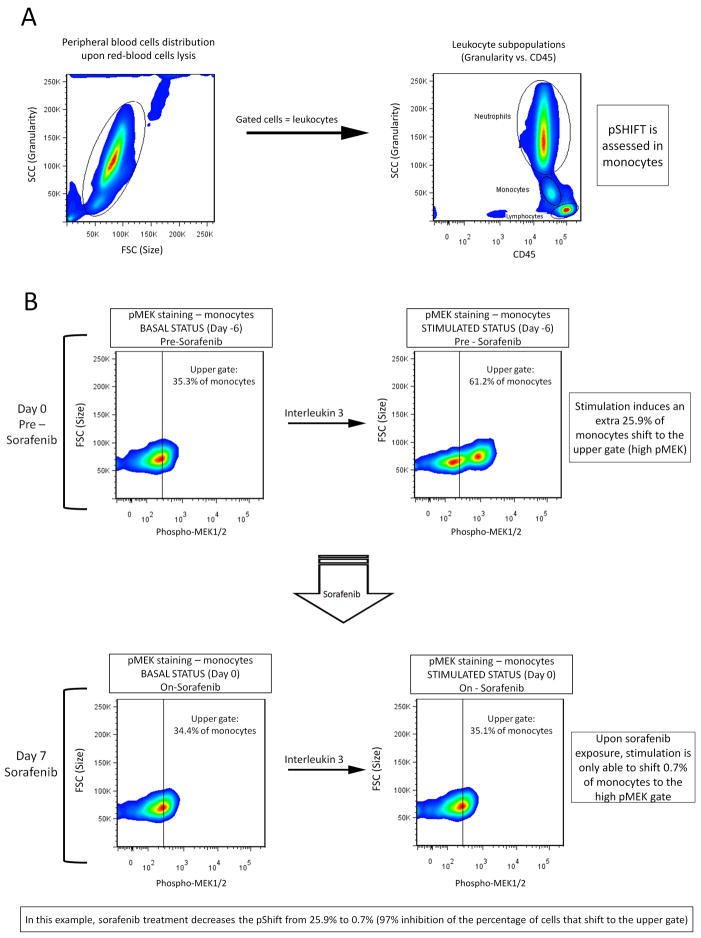
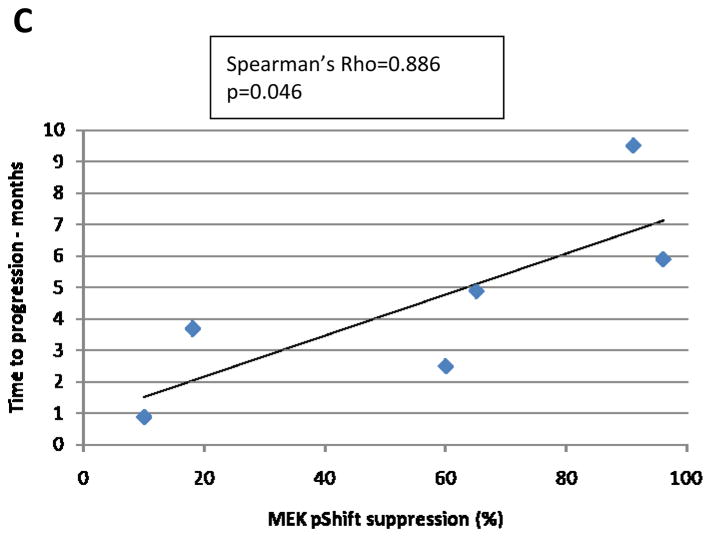
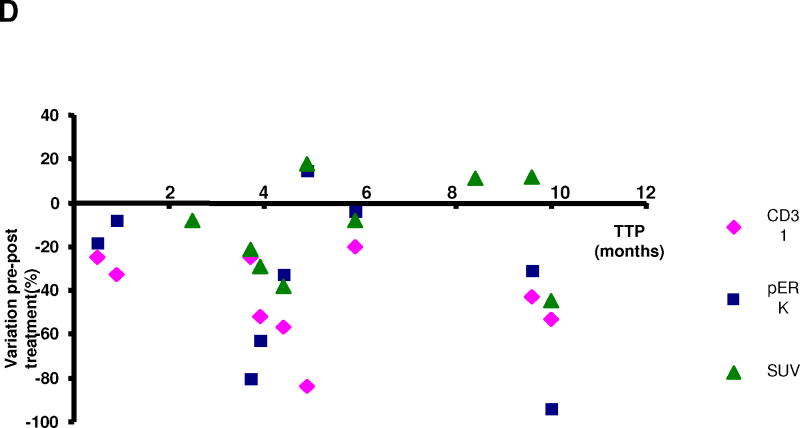
The aims of this study were to further define the safety of sorafenib and erlotinib, given at their full approved monotherapy doses, and to correlate pharmacokinetic and pharmacodynamic markers with clinical outcome. In addition, a novel pharmacodynamic marker based on the real-time measurement of RAF signal transduction capacity (STC) is described. Sorafenib was administered alone for a 1-week run-in period, and then both drugs were given together continuously. RAF STC was assessed in peripheral blood monocytes prior to erlotinib initiation. Epidermal growth factor receptor (EGFR) expression and K-RAS mutations were measured in archival tumor samples. Changes in pERK and CD31 were determined in fresh tumor biopsies obtained pretreatment, prior to erlotinib dosing, and during the administration of both drugs. In addition, positron emission tomography-computed tomography scans and pharmacokinetic assessments were done. Eleven patients received a total of 57 cycles (median, 5; range, 1-10). Only four patients received full doses of both drugs for the entire study course, with elevation of liver enzymes being the main reason for dose reductions and delays. Among 10 patients evaluable for response, 8 experienced tumor stabilization of >or=4 cycles. Pharmacokinetic analysis revealed no significant interaction of erlotinib with sorafenib. Sorafenib-induced decrease in RAF-STC showed statistically significant correlation with time-to-progression in seven patients. Other pharmacodynamic markers did not correlate with clinical outcome. This drug combination resulted in promising clinical activity in solid tumor patients although significant toxicity warrants close monitoring. RAF-STC deserves further study as a predictive marker for sorafenib.
Conflict of interest statement
Miguel Quintela-Fandino: has conducted research funded by Bayer Pharmaceuticals.
Eric X. Chen: has received honoraria from and conducted research funded by Roche Pharmaceuticals.
Ming Tsao: has exerted compensated advisory role for and received honoraria from Roche Pharmaceuticals.
Lillian L. Siu: has conducted research funded by Bayer Pharmaceuticals.
Figures
References
-
- Moyer JD, Barbacci EG, Iwata KK, et al. Induction of apoptosis and cell cycle arrest by CP-358,774, an inhibitor of epidermal growth factor receptor tyrosine kinase. Cancer Res. 1997;57:4838–4848. - PubMed
-
- Pollack VA, Savage DM, Baker DA, et al. Inhibition of epidermal growth factor receptor-associated tyrosine phosphorylation in human carcinomas with CP-358,774: dynamics of receptor inhibition in situ and antitumor effects in athymic mice. J Pharmacol Exp Ther. 1999;291:739–748. - PubMed
-
- Adnane L, Trail PA, Taylor I, Wilhelm SM. Sorafenib (BAY 43-9006, Nexavar((R))), a Dual-Action Inhibitor That Targets RAF/MEK/ERK Pathway in Tumor Cells and Tyrosine Kinases VEGFR/PDGFR in Tumor Vasculature. Methods Enzymol. 2005;407:597–612. - PubMed
-
- Wilhelm SM, Carter C, Tang L, et al. BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res. 2004;64:7099–7109. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
