

Imaging the pericardium: appearances on ECG-gated 64-detector row cardiac computed tomography
- PMID: 20197434
- PMCID: PMC3473560
- DOI: 10.1259/bjr/55699491
Imaging the pericardium: appearances on ECG-gated 64-detector row cardiac computed tomography
Abstract
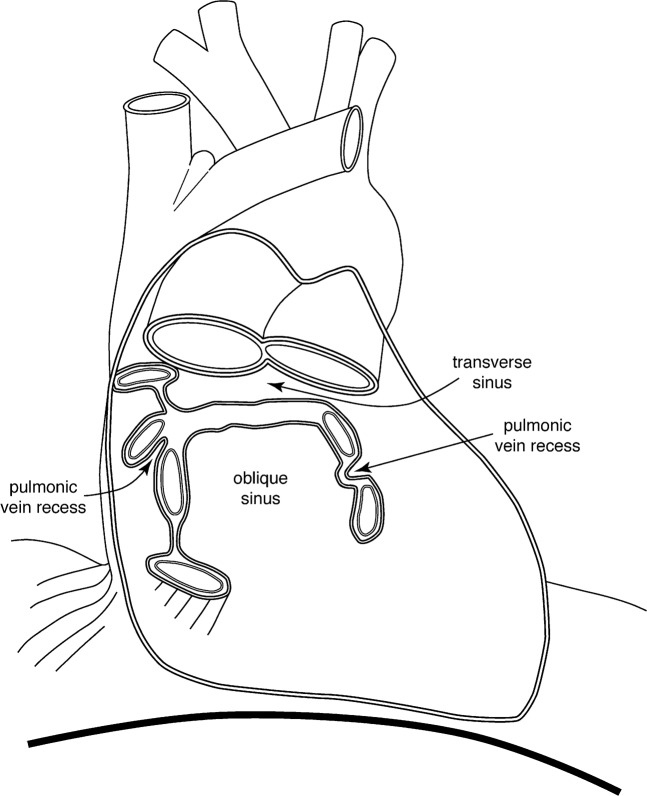
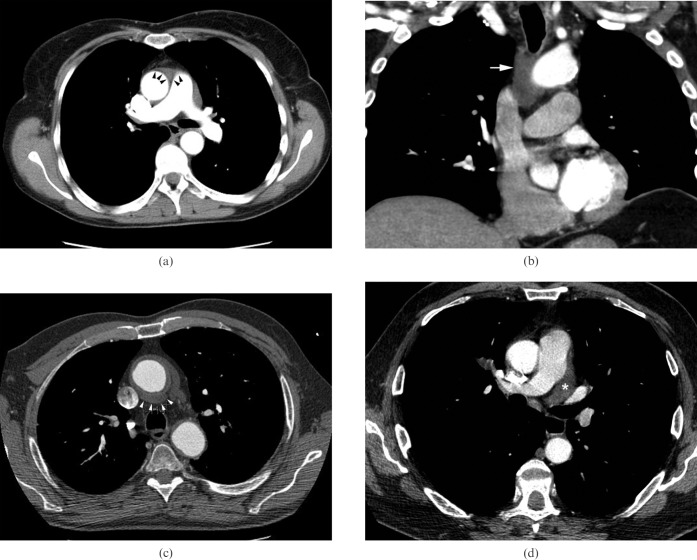
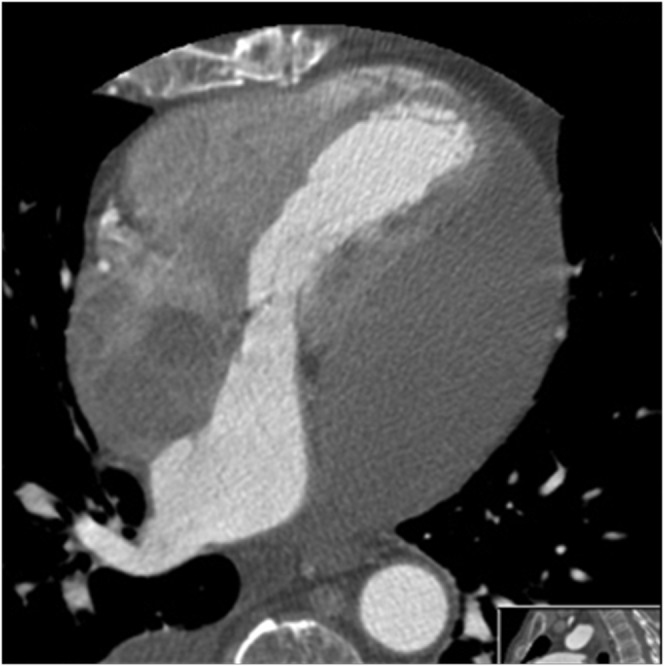
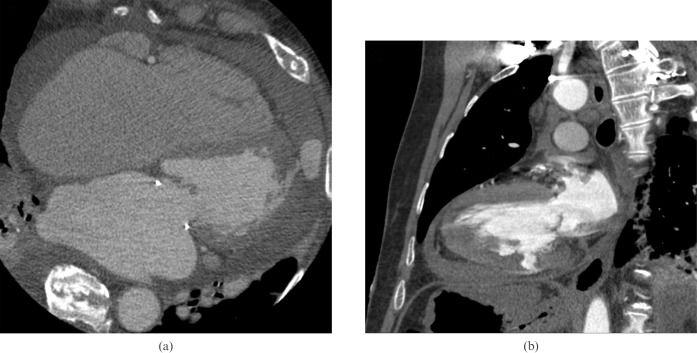
Multidetector row computed tomography (MDCT) with its high spatial and temporal resolution has now become an established and complementary method for cardiac imaging. It can now be used reliably to exclude significant coronary artery disease and delineate complex coronary artery anomalies, and has become a valuable problem-solving tool. Our experience with MDCT imaging suggests that it is clinically useful for imaging the pericardium. It is important to be aware of the normal anatomy of the pericardium and not mistake normal variations for pathology. The pericardial recesses are visible in up to 44% of non-electrocardiogram (ECG)-gated MDCT images. Abnormalities of the pericardium can now be identified with increasing certainty on 64-detector row CT; they may be the key to diagnosis and therefore must not be overlooked. This educational review of the pericardium will cover different imaging techniques, with a significant emphasis on MDCT. We have a large research and clinical experience of ECG-gated cardiac CT and will demonstrate examples of pericardial recesses, their variations and a wide variety of pericardial abnormalities and systemic conditions affecting the pericardium. We give a brief relevant background of the conditions and reinforce the key imaging features. We aim to provide a pictorial demonstration of the wide variety of abnormalities of the pericardium and the pitfalls in the diagnosis of pericardial disease.
Figures


Similar articles
-
Multimodality Imaging for the Assessment of Pericardial Diseases.Curr Cardiol Rep. 2019 Apr 16;21(5):41. doi: 10.1007/s11886-019-1115-y. Curr Cardiol Rep. 2019. PMID: 30993456 Review.
-
Pericardial disease--anatomy and function.Br J Radiol. 2011 Dec;84 Spec No 3(Spec Iss 3):S324-37. doi: 10.1259/bjr/16168253. Br J Radiol. 2011. PMID: 22723538 Free PMC article. Review.
-
Computed tomography of the pericardium and pericardial disease.J Cardiovasc Comput Tomogr. 2010 Jan-Feb;4(1):3-18. doi: 10.1016/j.jcct.2010.01.004. Epub 2010 Jan 11. J Cardiovasc Comput Tomogr. 2010. PMID: 20159622
-
Computed tomography and magnetic resonance imaging of the pericardium.Radiographics. 1989 Jul;9(4):633-49. doi: 10.1148/radiographics.9.4.2756190. Radiographics. 1989. PMID: 2756190
-
Imaging of Pericardial Disease.Radiol Clin North Am. 2019 Jan;57(1):179-199. doi: 10.1016/j.rcl.2018.09.001. Radiol Clin North Am. 2019. PMID: 30454812 Review.
Cited by
-
Extensive pericardial calcification secondary to radiotherapy, causing mixed constrictive-restrictive pathology.BJR Case Rep. 2017 Jul 29;3(4):20170036. doi: 10.1259/bjrcr.20170036. eCollection 2017. BJR Case Rep. 2017. PMID: 30363214 Free PMC article.
-
Multimodality Imaging for the Assessment of Pericardial Diseases.Curr Cardiol Rep. 2019 Apr 16;21(5):41. doi: 10.1007/s11886-019-1115-y. Curr Cardiol Rep. 2019. PMID: 30993456 Review.
-
Epicardial interventions in electrophysiology.Circulation. 2012 Oct 2;126(14):1752-69. doi: 10.1161/CIRCULATIONAHA.111.060327. Circulation. 2012. PMID: 23027811 Free PMC article. Review. No abstract available.
-
Hemopericardium in the acute clinical setting: Are we ready for a tailored management approach on the basis of MDCT findings?Radiol Med. 2021 Apr;126(4):527-543. doi: 10.1007/s11547-020-01303-x. Epub 2020 Nov 2. Radiol Med. 2021. PMID: 33136215 Review.
-
Cardiac computed tomography in cardio-oncology: an update on recent clinical applications.Eur Heart J Cardiovasc Imaging. 2021 Mar 22;22(4):397-405. doi: 10.1093/ehjci/jeaa351. Eur Heart J Cardiovasc Imaging. 2021. PMID: 33555007 Free PMC article. Review.
References
-
- Kini S, Bis KG, Weaver L. Normal and variant coronary arterial and venous anatomy on high-resolution CT angiography. AJR Am J 2007;188:1665–74 - PubMed
-
- Cury RC, Nieman K, Shapiro MD, Nasir K, Cury RC, Brady TJ. Comprehensive cardiac CT study: evaluation of coronary arteries, left ventricular function and myocardial perfusion — is it possible? J Nuc Cardiol 2007;14:229–43 - PubMed
-
- Broderick LS, Brooks GN, Kuhlman JE. Anatomic pitfalls of the heart and pericardium. Radiographics 2005;25:441–53 - PubMed
-
- Bull RK, Edwards PD, Dixon AK. CT dimensions of the normal pericardium. Br J Radiol 1998;71:923–5 - PubMed
-
- Truong MT, Erasmus JJ, Gladish GW, Sabloff BS, Marom EM, Madewell JE, et al. Anatomy of pericardial recesses on multidetector CT: implications for oncologic imaging. AJR 2003;181:1109–13 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
