

Miliary tuberculosis: a comparison of CT findings in HIV-seropositive and HIV-seronegative patients
- PMID: 20197435
- PMCID: PMC3473551
- DOI: 10.1259/bjr/95169618
Miliary tuberculosis: a comparison of CT findings in HIV-seropositive and HIV-seronegative patients
Abstract
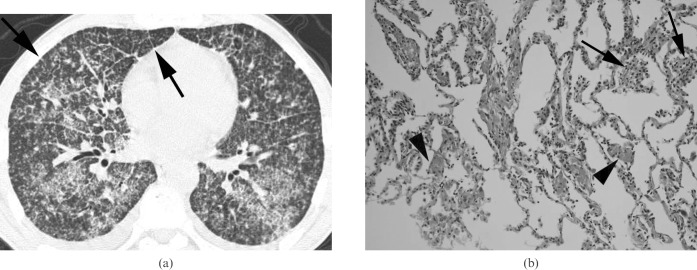
The aim of this study was to determine the differences in CT findings of miliary tuberculosis in patients with and without HIV infection. Two radiologists reviewed retrospectively the CT findings of 15 HIV-seropositive and 14 HIV-seronegative patients with miliary tuberculosis. The decisions on the findings were reached by consensus. Statistical analysis was performed using the chi2 test, Mann-Whitney U-test and Fisher's exact test. All of the HIV-seropositive and -seronegative patients had small nodules and micronodules distributed randomly throughout both lungs. HIV-seropositive patients had a higher prevalence of interlobular septal thickening (p = 0.017), necrotic lymph nodes (p = 0.005) and extrathoracic involvement (p = 0.040). The seropositive patients had a lower prevalence of large nodules (p = 0.031). In conclusion, recognition of the differences in the radiological findings between HIV-seropositive and -seronegative patients may help in the establishment of an earlier diagnosis of immune status in patients with miliary tuberculosis.
Figures


References
-
- Gelb AF, Leffler C, Brewin A, Mascatello V, Lyons HA. Miliary tuberculosis. Am Rev Respir Dis 1973;108:1327–33 - PubMed
-
- Geppert EF, Leff A. The pathogenesis of pulmonary and miliary tuberculosis. Arch Intern Med 1979;139:1381–3 - PubMed
-
- Sahn SA, Neff TA. Miliary tuberculosis. Am J Med 1974;56:494–505 - PubMed
-
- Sunderam G, McDonald RJ, Maniatis T, Oleske J, Kapila R, Reichman LB. Tuberculosis as a manifestation of the acquired immunodeficiency syndrome (AIDS). JAMA 1986;256:362–6 - PubMed
-
- World HealthOrganization Programmes and Projects. Tuberculosis. Address TB/HIV, MDR/XDR-TB and Other Challenges. 2007. Available from: http:\\www.who.int\tb\challenges\hiv\facts\en\ [Accessed 3 July 2009]
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
