

Is irritable bowel syndrome a diagnosis of exclusion?: a survey of primary care providers, gastroenterologists, and IBS experts
- PMID: 20197761
- PMCID: PMC2887205
- DOI: 10.1038/ajg.2010.47
Is irritable bowel syndrome a diagnosis of exclusion?: a survey of primary care providers, gastroenterologists, and IBS experts
Abstract
Objectives: Guidelines emphasize that irritable bowel syndrome (IBS) is not a diagnosis of exclusion and encourage clinicians to make a positive diagnosis using the Rome criteria alone. Yet many clinicians are concerned about overlooking alternative diagnoses. We measured beliefs about whether IBS is a diagnosis of exclusion, and measured testing proclivity between IBS experts and community providers.
Methods: We developed a survey to measure decision-making in two standardized patients with Rome III-positive IBS, including IBS with diarrhea (D-IBS) and IBS with constipation (C-IBS). The survey elicited provider knowledge and beliefs about IBS, including testing proclivity and beliefs regarding IBS as a diagnosis of exclusion. We surveyed nurse practitioners, primary care physicians, community gastroenterologists, and IBS experts.
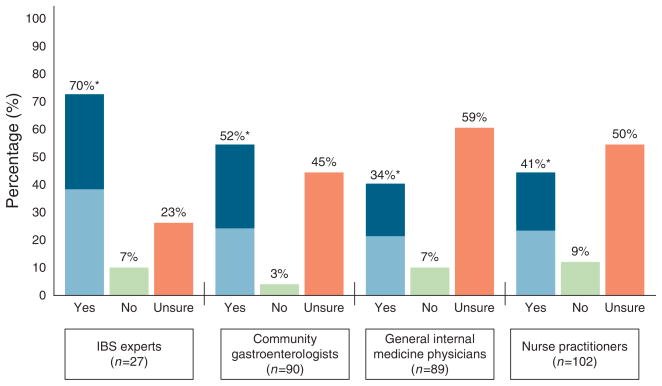
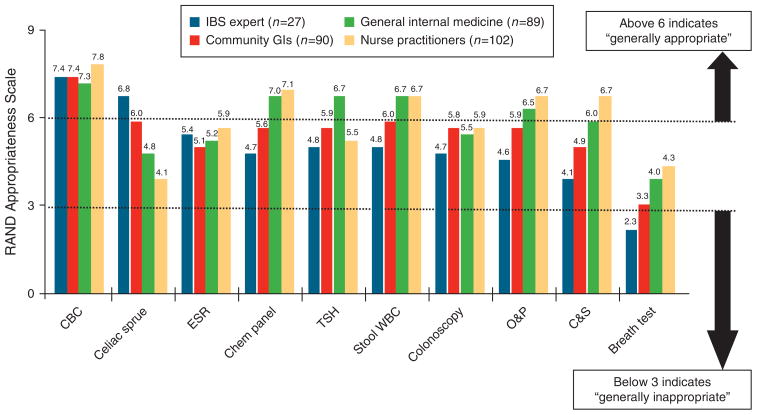
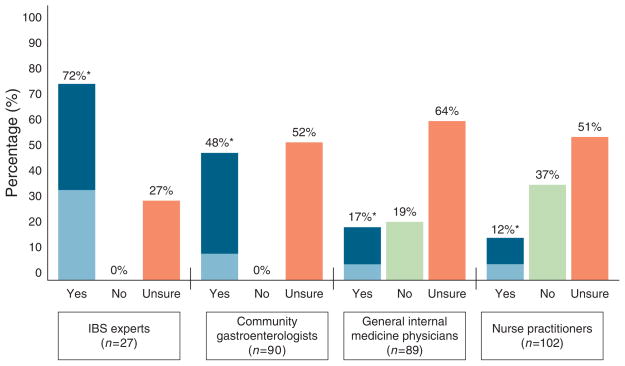
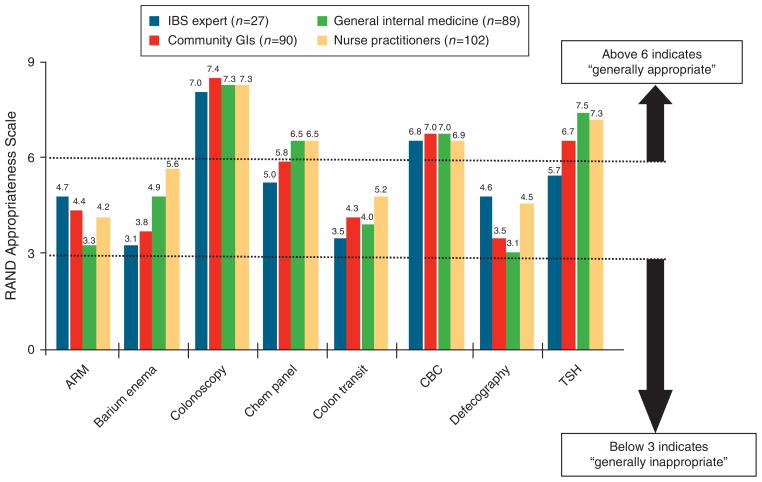
Results: Experts were less likely than nonexperts to endorse IBS as a diagnosis of exclusion (8 vs. 72%; P<0.0001). In the D-IBS vignette, experts were more likely to make a positive diagnosis of IBS (67 vs. 38%; P<0.001), to perform fewer tests (2.0 vs. 4.1; P<0.01), and to expend less money on testing (US$297 vs. $658; P<0.01). Providers who believed IBS is a diagnosis of exclusion ordered 1.6 more tests and consumed $364 more than others (P<0.0001). Experts only rated celiac sprue screening and complete blood count as appropriate in D-IBS; nonexperts rated most tests as appropriate. Parallel results were found in the C-IBS vignette.
Conclusions: Most community providers believe IBS is a diagnosis of exclusion; this belief is associated with increased resource use. Experts comply more closely with guidelines to diagnose IBS with minimal testing. This disconnect suggests that better implementation of guidelines is warranted to minimize variation and improve cost-effectiveness of care.
Conflict of interest statement
Figures
Comment in
-
[Irritable bowel syndrome: to scope or not to scope?].Z Gastroenterol. 2010 Aug;48(8):852-3. doi: 10.1055/s-0029-1245564. Epub 2010 Aug 4. Z Gastroenterol. 2010. PMID: 20687023 German. No abstract available.
Similar articles
-
Diagnosing and managing irritable bowel syndrome with predominant diarrhoea in clinical practice: online survey among gastroenterologists and general practitioners.Acta Gastroenterol Belg. 2024 Apr-Jun;87(2):229-234. doi: 10.51821/87.2.12586. Acta Gastroenterol Belg. 2024. PMID: 39210754
-
Perceptions and Practices of Primary Care Providers in Europe and the US in the Diagnosis and Treatment of Irritable Bowel Syndrome: A Multinational Survey.Neurogastroenterol Motil. 2025 Feb;37(2):e14967. doi: 10.1111/nmo.14967. Epub 2024 Nov 20. Neurogastroenterol Motil. 2025. PMID: 39568286 Free PMC article.
-
Diagnosis of Irritable Bowel Syndrome: Primary Care Physicians Compared with Gastroenterologists.Clin Med Res. 2023 Sep;21(3):129-135. doi: 10.3121/cmr.2023.1817. Clin Med Res. 2023. PMID: 37985167 Free PMC article.
-
ACG Clinical Guideline: Management of Irritable Bowel Syndrome.Am J Gastroenterol. 2021 Jan 1;116(1):17-44. doi: 10.14309/ajg.0000000000001036. Am J Gastroenterol. 2021. PMID: 33315591
-
A symptom-based approach to making a positive diagnosis of irritable bowel syndrome with constipation.Int J Clin Pract. 2006 Jan;60(1):57-63. doi: 10.1111/j.1368-5031.2005.00744.x. Int J Clin Pract. 2006. PMID: 16409429 Review.
Cited by
-
Microscopic colitis - a missed diagnosis in diarrhea-predominant irritable bowel syndrome.Maedica (Bucur). 2012 Jan;7(1):3-9. Maedica (Bucur). 2012. PMID: 23118812 Free PMC article.
-
Patient-Provider Communication: The Key to Improving IBS-C Management.Gastroenterol Hepatol (N Y). 2025 Jan;21(1):28-39. Gastroenterol Hepatol (N Y). 2025. PMID: 39897339 Free PMC article. No abstract available.
-
Multiple rather than specific autoantibodies were identified in irritable bowel syndrome with HuProt™ proteome microarray.Front Physiol. 2022 Oct 3;13:1010069. doi: 10.3389/fphys.2022.1010069. eCollection 2022. Front Physiol. 2022. PMID: 36262261 Free PMC article.
-
Construction and validation of a questionnaire distinguishing a chronic abdominal wall pain syndrome from irritable bowel syndrome.Frontline Gastroenterol. 2012 Oct;3(4):288-294. doi: 10.1136/flgastro-2012-100207. Epub 2012 Jul 26. Frontline Gastroenterol. 2012. PMID: 23914291 Free PMC article.
-
Approaching patients with irritable bowel syndrome.F1000 Med Rep. 2010 Jul 14;2:50. doi: 10.3410/M2-50. F1000 Med Rep. 2010. PMID: 20948834 Free PMC article.
References
-
- Longstreth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. Gastroenterology. 2006;130:1480–91. - PubMed
-
- Spiegel BM. The burden of IBS: looking at metrics. Curr Gastroenterol Rep. 2009;11:265–9. - PubMed
-
- Spiegel B. Do physicians follow evidence-based guidelines in the diagnostic work-up of IBS? Nat Clin Pract Gastroenterol Hepatol. 2007;4:296–7. - PubMed
-
- Cash BD, Schoenfeld P, Chey WD. The utility of diagnostic tests in irritable bowel syndrome patients: a systematic review. Am J Gastroenterol. 2002;97:2812–9. - PubMed
-
- Cash BD, Schoenfeld P, Chey WD. The utility of diagnostic tests in irritable bowel syndrome patients: a systematic review. Am J Gastroenterol. 2002;97:2812–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
