

Preferences for colorectal cancer screening strategies: a discrete choice experiment
- PMID: 20197766
- PMCID: PMC2844026
- DOI: 10.1038/sj.bjc.6605566
Preferences for colorectal cancer screening strategies: a discrete choice experiment
Abstract
Background: Guidelines underline the role of individual preferences in the selection of a screening test, as insufficient evidence is available to recommend one screening test over another. We conducted a study to determine the preferences of individuals and to predict uptake for colorectal cancer (CRC) screening programmes using various screening tests.
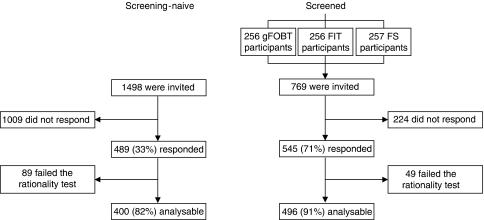
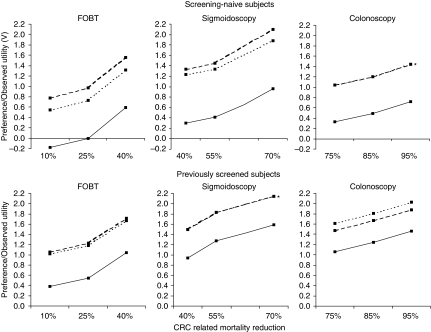
Methods: A discrete choice experiment (DCE) questionnaire was distributed among naive subjects, yet to be screened, and previously screened subjects, aged 50-75 years. Subjects were asked to choose between scenarios on the basis of faecal occult blood test (FOBT), flexible sigmoidoscopy (FS), total colonoscopy (TC) with various test-specific screening intervals and mortality reductions, and no screening (opt-out).
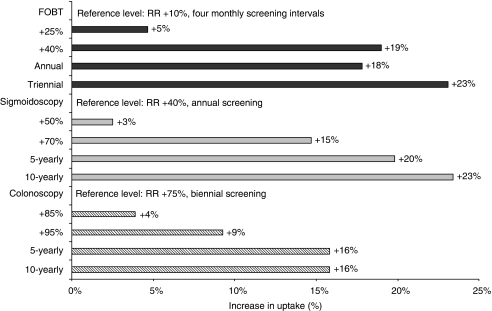
Results: In total, 489 out of 1498 (33%) screening-naïve subjects (52% male; mean age+/-s.d. 61+/-7 years) and 545 out of 769 (71%) previously screened subjects (52% male; mean age+/-s.d. 61+/-6 years) returned the questionnaire. The type of screening test, screening interval, and risk reduction of CRC-related mortality influenced subjects' preferences (all P<0.05). Screening-naive and previously screened subjects equally preferred 5-yearly FS and 10-yearly TC (P=0.24; P=0.11), but favoured both strategies to annual FOBT screening (all P-values <0.001) if, based on the literature, realistic risk reduction of CRC-related mortality was applied. Screening-naive and previously screened subjects were willing to undergo a 10-yearly TC instead of a 5-yearly FS to obtain an additional risk reduction of CRC-related mortality of 45% (P<0.001).
Conclusion: These data provide insight into the extent by which interval and risk reduction of CRC-related mortality affect preferences for CRC screening tests. Assuming realistic test characteristics, subjects in the target population preferred endoscopic screening over FOBT screening, partly, due to the more favourable risk reduction of CRC-related mortality by endoscopy screening. Increasing the knowledge of potential screenees regarding risk reduction by different screening strategies is, therefore, warranted to prevent unrealistic expectations and to optimise informed choice.
Figures
References
-
- Commission of the European Communities. Proposal for a Council Recommendation on Cancer Screening, 2003/0093 (CNS). Brussel, 5 May 2003
-
- Dolan P (1997) Modeling valuations for EuroQol health states. Med Care 35: 1095–1108 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
