

The clinical spectrum of Blake's pouch cyst: report of six illustrative cases
- PMID: 20198375
- PMCID: PMC2903702
- DOI: 10.1007/s00381-010-1085-2
The clinical spectrum of Blake's pouch cyst: report of six illustrative cases
Abstract
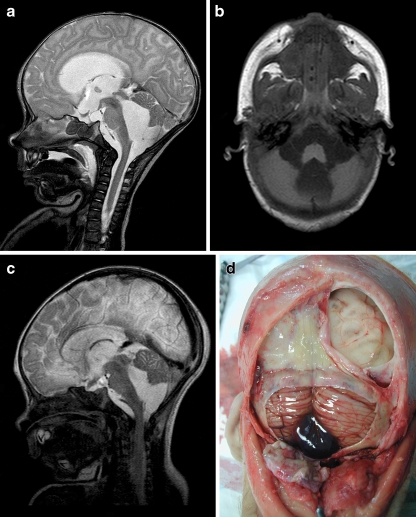
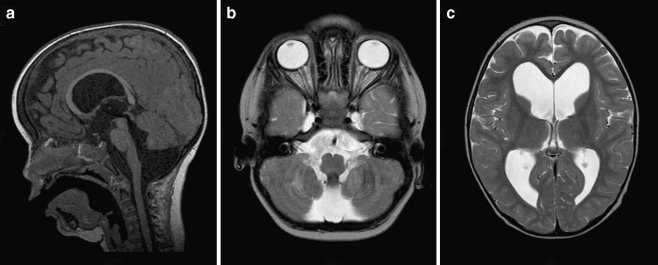
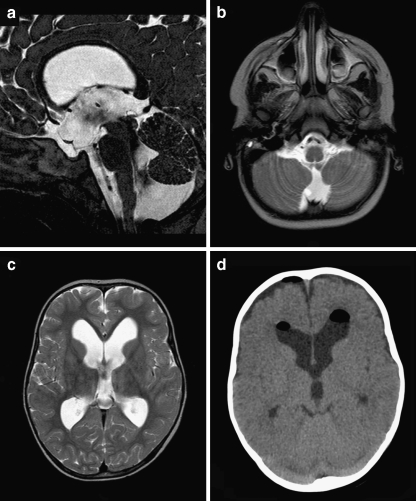
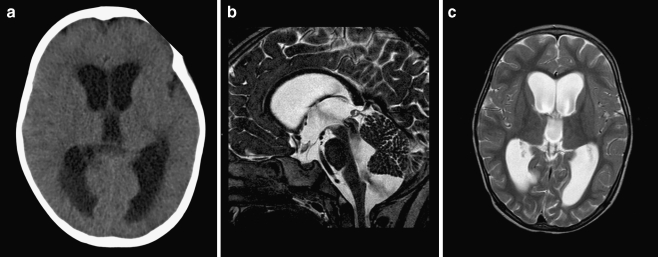
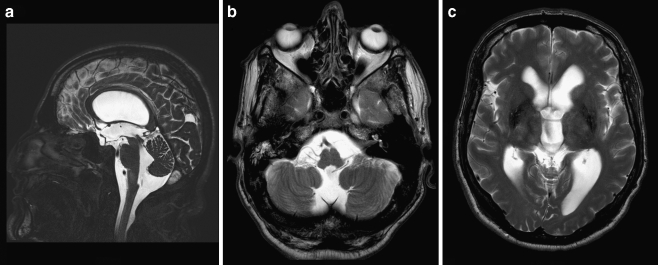
Introduction: Although Blake's pouch cyst (BPC) is frequently mentioned in the spectrum of posterior fossa cysts and cystlike malformations since its first description in 1996, its natural history, clinical presentation, specific imaging characteristics, optimal treatment, and outcome are relatively unknown. Consequently, BPC may still be underdiagnosed. We therefore report six cases ranging from a fatal hydrocephalus in a young boy, over an increasing head circumference with or without impaired neurological development in two infants, to a decompensating hydrocephalus at an advanced age.
Discussion: We focus on their radiological uniformity, which should help making the correct diagnosis, and widely variable clinical presentation, which includes adult cases as well. Differentiating BPC from other posterior fossa cysts and cystlike malformations and recognizing the accompanying hydrocephalus are essentially noncommunicating, not only have important implications on clinical management but also on genetic counseling, which is unnecessary in case of BPC. In our experience, endoscopic third ventriculostomy is a safe and effective treatment option, avoiding the risks and added morbidity of open surgery, as well as many shunt-related problems.
Figures

Comment in
-
Comment to the paper (CNS-09-0420) "The clinical spectrum of Blake's pouch cyst: report of 6 illustrative cases".Childs Nerv Syst. 2010 Aug;26(8):1065-6. doi: 10.1007/s00381-010-1116-z. Epub 2010 Mar 10. Childs Nerv Syst. 2010. PMID: 20217096 No abstract available.
-
The clinical spectrum of Blake's pouch cyst.Childs Nerv Syst. 2010 Dec;26(12):1665; author reply 1167-8. doi: 10.1007/s00381-010-1293-9. Epub 2010 Oct 2. Childs Nerv Syst. 2010. PMID: 20890607 No abstract available.
References
-
- Barkovich AJ, Kjos BO, Norman D, Edwards MS. Revised classification of posterior fossa cysts and cystlike malformations based on the results of multiplanar MR imaging. AJNR. 1989;10:977–988. - PubMed
-
- Barkovich AJ. Pediatric neuroimaging. 2. New York: Raven; 1994. pp. 177–275.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
