

Use of EEG monitoring and management of non-convulsive seizures in critically ill patients: a survey of neurologists
- PMID: 20198513
- PMCID: PMC2944658
- DOI: 10.1007/s12028-010-9337-2
Use of EEG monitoring and management of non-convulsive seizures in critically ill patients: a survey of neurologists
Abstract
Background: Continuous EEG monitoring (cEEG) of critically ill patients is frequently utilized to detect non-convulsive seizures (NCS) and status epilepticus (NCSE). The indications for cEEG, as well as when and how to treat NCS, remain unclear. We aimed to describe the current practice of cEEG in critically ill patients to define areas of uncertainty that could aid in designing future research.
Methods: We conducted an international survey of neurologists focused on cEEG utilization and NCS management.
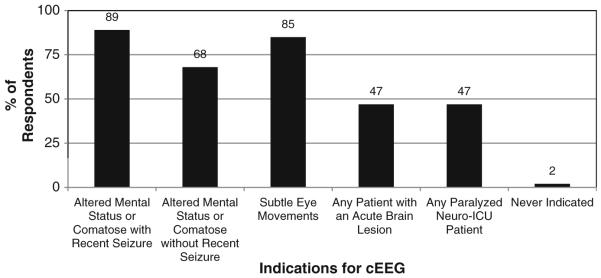
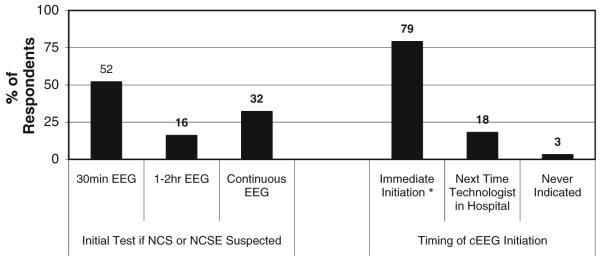
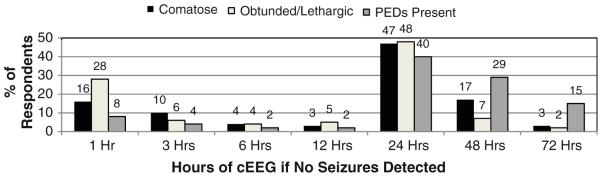
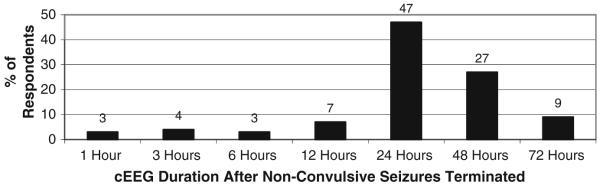
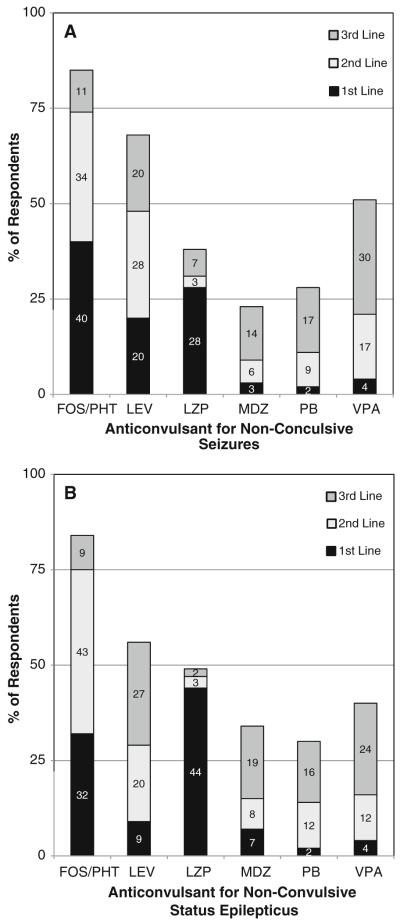
Results: Three-hundred and thirty physicians completed the survey. 83% use cEEG at least once per month and 86% manage NCS at least five times per year. The use of cEEG in patients with altered mental status was common (69%), with higher use if the patient had a prior convulsion (89%) or abnormal eye movements (85%). Most respondents would continue cEEG for 24 h. If NCS or NCSE is identified, the most common anticonvulsants administered were phenytoin/fosphenytoin, lorazepam, or levetiracetam, with slightly more use of levetiracetam for NCS than NCSE.
Conclusions: Continuous EEG monitoring (cEEG) is commonly employed in critically ill patients to detect NCS and NCSE. However, there is substantial variability in current practice related to cEEG indications and duration and to management of NCS and NCSE. The fact that such variability exists in the management of this common clinical problem suggests that further prospective study is needed. Multiple points of uncertainty are identified that require investigation.
Figures
References
-
- Friedman D, Claassen J, Hirsch LJ. Continuous electroencephalogram monitoring in the intensive care unit. Anesth Analg. 2009;109:506–23. - PubMed
-
- Kurtz P, Hanafy KA, Claassen J. Continuous EEG monitoring: is it ready for prime time? Curr Opin Crit Care. 2009;15:99–109. - PubMed
-
- Claassen J, Mayer SA, Kowalski RG, Emerson RG, Hirsch LJ. Detection of electrographic seizures with continuous EEG monitoring in critically ill patients. Neurology. 2004;62:1743–8. - PubMed
-
- Jette N, Claassen J, Emerson RG, Hirsch LJ. Frequency and predictors of nonconvulsive seizures during continuous electroencephalographic monitoring in critically ill children. Arch Neurol. 2006;63:1750–5. - PubMed
-
- Vespa PM, Nenov V, Nuwer MR. Continuous EEG monitoring in the intensive care unit: early findings and clinical efficacy. J Clin Neurophysiol. 1999;16:1–13. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
