

The role of radiology in head and neck tumours in children
- PMID: 20199940
- PMCID: PMC2842180
- DOI: 10.1102/1470-7330.2010.0003
The role of radiology in head and neck tumours in children
Abstract
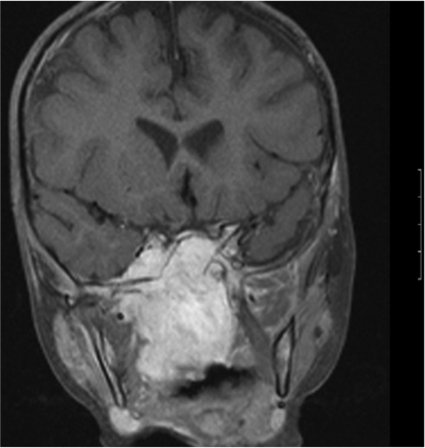
Head and neck malignancy is rare in children. However, distinguishing malignant tumours from the more common and numerous benign causes of neck masses in childhood is crucial as many malignant conditions have an excellent prognosis with appropriate oncological management. Ultrasound, computed tomography and magnetic resonance imaging all have crucial roles in the diagnosis of head and neck malignancy in children and there is an emerging role for positron emission tomography, particularly in the management and follow-up of lymphoma. We describe the imaging appearances of the common malignant tumours arising in the extracranial head and neck in children, focusing on lymphoma, rhabdomyosarcoma and nasopharyngeal carcinoma. The clinical presentation and radiological appearances of benign tumours in the head and neck in children may overlap with those seen in malignant disease. We describe the imaging appearances of juvenile angiofibroma, vascular abnormalities involving the extracranial head and neck and cervical teratomas. Advances in both imaging techniques and cancer staging systems, many of the latter aimed at avoiding over-treatment and treatment-related complications, will lead to an increasingly central role for imaging in childhood head and neck cancer.
Figures











Similar articles
-
Imaging of head and neck neoplasms in children.Pediatr Radiol. 2010 Apr;40(4):499-509. doi: 10.1007/s00247-009-1526-9. Pediatr Radiol. 2010. PMID: 20225112
-
Pediatric head and neck rhabdomyosarcoma; the role of MRI in differentiation from other common pediatric malignant head and neck tumors.Turk J Pediatr. 2022;64(3):519-530. doi: 10.24953/turkjped.2021.4600. Turk J Pediatr. 2022. PMID: 35899565
-
Tumors and tumor-like lesions of the neck: from childhood to adult.Eur Radiol. 2004 Mar;14 Suppl 4:L155-65. doi: 10.1007/s00330-003-2035-0. Eur Radiol. 2004. PMID: 14752572 Review.
-
Extracranial head and neck neoplasms: role of imaging.Cancer Treat Res. 2008;143:93-117. doi: 10.1007/978-0-387-75587-8_4. Cancer Treat Res. 2008. PMID: 18619215 Review. No abstract available.
-
Modern Radiology in the Management of Head and Neck Cancer.Clin Oncol (R Coll Radiol). 2016 Jul;28(7):440-50. doi: 10.1016/j.clon.2016.03.003. Epub 2016 May 4. Clin Oncol (R Coll Radiol). 2016. PMID: 27156741
Cited by
-
The influence of preformed metal crowns versus zirconia crowns on the diagnostic quality of magnetic resonance images.Eur Arch Paediatr Dent. 2025 Feb;26(1):109-117. doi: 10.1007/s40368-024-00971-x. Epub 2024 Nov 13. Eur Arch Paediatr Dent. 2025. PMID: 39538095
-
Juvenile Nasopharyngeal Angiofibroma: Magnetic Resonance Imaging Findings.J Belg Soc Radiol. 2016 Jun 1;100(1):63. doi: 10.5334/jbr-btr.1090. J Belg Soc Radiol. 2016. PMID: 30038985 Free PMC article.
-
Nasopharyngeal carcinoma in a 15-year-old: A rare pediatric tumor.Radiol Case Rep. 2025 Jun 12;20(9):4305-4311. doi: 10.1016/j.radcr.2025.05.022. eCollection 2025 Sep. Radiol Case Rep. 2025. PMID: 40575367 Free PMC article.
-
Magnetic resonance imaging versus computed tomography and different imaging modalities in evaluation of sinonasal neoplasms diagnosed by histopathology.Clin Med Insights Ear Nose Throat. 2013 Jun 26;6:9-15. doi: 10.4137/CMENT.S10678. eCollection 2013. Clin Med Insights Ear Nose Throat. 2013. PMID: 24179408 Free PMC article.
-
Can preoperative computed tomography predict tissue origin of primary maxillary cancer?Medicine (Baltimore). 2016 Oct;95(40):e4831. doi: 10.1097/MD.0000000000004831. Medicine (Baltimore). 2016. PMID: 27749536 Free PMC article.
References
-
- Boring CC, Squires TS, Tong T. Cancer Statistics, 1993. CA Cancer J Clin. 1993;43:7–26. doi:10.3322/canjclin.43.1.7. PMid:8422609. - DOI - PubMed
-
- Imhof H, Czerny C, Hormann M, Krestan C. Tumors and tumor-like lesions of the neck: from childhood to adult. European Radiology. 2004;14:L155–65. - PubMed
-
- Hermans R, editor. Head and neck cancer imaging. Berlin, Heidelberg: Springer-Verlag; 2006.
-
- Abdel Razek A, Gaballa G, Elhawarey G, Megahed A, Hafez M, Nada N. Characterization of pediatric head and neck masses with diffusion-weighted MR imaging. Eur Radiol. 2009;19:201–8. doi:10.1007/s00330-008-1123-6. PMid:18704436. - DOI - PubMed
-
- Jadvar H, Connolly L, Fahey F, Shulkin B. PET and PET/CT in pediatric oncology. Semin Nucl Med. 2007;37:316–31. doi:10.1053/j.semnuclmed.2007.04.001. PMid:17707239. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases