

Cardiac PET-CT: advanced hybrid imaging for the detection of coronary artery disease
- PMID: 20200615
- PMCID: PMC2828569
- DOI: 10.1007/BF03091744
Cardiac PET-CT: advanced hybrid imaging for the detection of coronary artery disease
Abstract
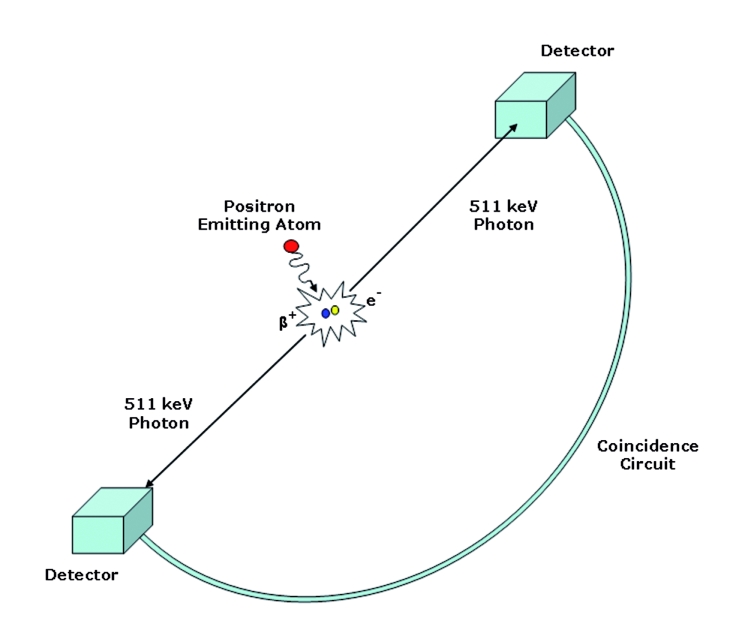
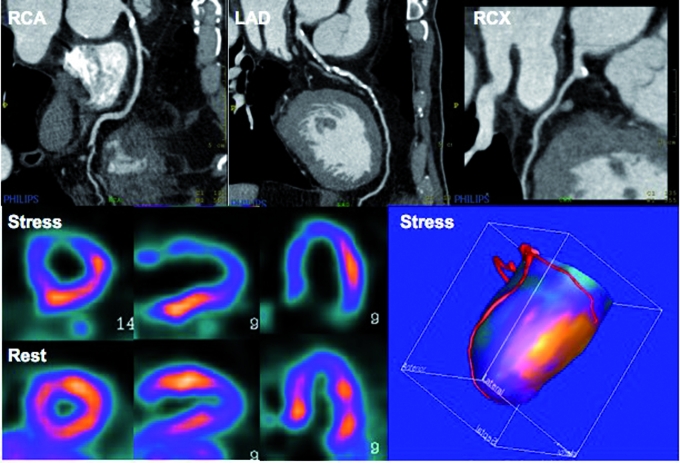
Hybrid imaging of positron emission tomography (PET) together with computed tomography (CT) is rapidly emerging. In cardiology, this new advanced hybrid imaging modality allows quantification of cardiac perfusion in combination with assessment of coronary anatomy within a single scanning session of less than 45 minutes. The near-simultaneous anatomical evaluation of coronary arteries using CT and corresponding functional status using PET provides a wealth of complementary information in patients who are being evaluated for (suspected) coronary artery disease, and could help guide clinical patient management in a novel manner. Clinical experience gained with this recently introduced advanced hybrid imaging tool, however, is still limited and its implementation into daily clinical practice remains largely unchartered territory. This review discusses principles of perfusion PET, its diagnostic accuracy, and potential clinical applications of cardiac PET-CT in patients with ischaemic heart disease. (Neth Heart J 2010;18:90-8.).
Keywords: Coronary Artery Disease; Positron-Emission Tomography; Tomography; X-Ray Computed.
Figures
References
-
- Knaapen P, Lubberink M. Cardiac positron emission tomography: myocardial perfusion and metabolism in clinical practice. Clin Res Cardiol. 2008;97:791–6. - PubMed
-
- Kaufmann PA, Camici PG. Myocardial blood flow measurement by PET: technical aspects and clinical applications. J Nucl Med. 2005;46:75–88. - PubMed
-
- Di Carli MF, Hachamovitch R. New technology for noninvasive evaluation of coronary artery disease. Circulation. 2007;115:1464–80. - PubMed
-
- Le Guludec D, Lautamaki R, Knuuti J, Bax JJ, Bengel FM. Present and future of clinical cardiovascular PET imaging in Europe a position statement by the European Council of Nuclear Cardiology (ECNC). Eur J Nucl Med Mol Imaging. 2008;35:1709–24. - PubMed
-
- Schroeder S, Achenbach S, Bengel F, Burgstahler C, Cademartiri F, de Feyter P, et al. Cardiac computed tomography: indications, applications, limitations, and training requirements: report of a Writing Group deployed by the Working Group Nuclear Cardiology and Cardiac CT of the European Society of Cardiology and the European Council of Nuclear Cardiology. Eur Heart J. 2008;29:531–56. - PubMed
LinkOut - more resources
Full Text Sources
Medical