

First experiences in the implementation of biometric technology to link data from Health and Demographic Surveillance Systems with health facility data
- PMID: 20200659
- PMCID: PMC2830803
- DOI: 10.3402/gha.v3i0.2120
First experiences in the implementation of biometric technology to link data from Health and Demographic Surveillance Systems with health facility data
Abstract
Background: In developing countries, Health and Demographic Surveillance Systems (HDSSs) provide a framework for tracking demographic and health dynamics over time in a defined geographical area. Many HDSSs co-exist with facility-based data sources in the form of Health Management Information Systems (HMIS). Integrating both data sources through reliable record linkage could provide both numerator and denominator populations to estimate disease prevalence and incidence rates in the population and enable determination of accurate health service coverage.
Objective: To measure the acceptability and performance of fingerprint biometrics to identify individuals in demographic surveillance populations and those attending health care facilities serving the surveillance populations.
Methodology: Two HDSS sites used fingerprint biometrics for patient and/or surveillance population participant identification. The proportion of individuals for whom a fingerprint could be successfully enrolled were characterised in terms of age and sex.
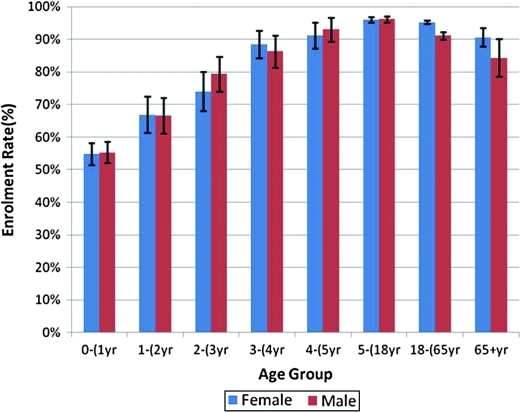
Results: Adult (18-65 years) fingerprint enrolment rates varied between 94.1% (95% CI 93.6-94.5) for facility-based fingerprint data collection at the Africa Centre site to 96.7% (95% CI 95.9-97.6) for population-based fingerprint data collection at the Agincourt site. Fingerprint enrolment rates in children under 1 year old (Africa Centre site) were only 55.1% (95% CI 52.7-57.4). By age 5, child fingerprint enrolment rates were comparable to those of adults.
Conclusion: This work demonstrates the feasibility of fingerprint-based individual identification for population-based research in developing countries. Record linkage between demographic surveillance population databases and health care facility data based on biometric identification systems would allow for a more comprehensive evaluation of population health, including the ability to study health service utilisation from a population perspective, rather than the more restrictive health service perspective.
Keywords: Health and Demographic Surveillance Systems; INDEPTH Network; biometrics; fingerprint; record linkage.
Figures
Similar articles
-
Implementation of Fingerprint Technology for Unique Patient Matching and Identification at an HIV Care and Treatment Facility in Western Kenya: Cross-sectional Study.J Med Internet Res. 2021 Dec 22;23(12):e28958. doi: 10.2196/28958. J Med Internet Res. 2021. PMID: 34941557 Free PMC article.
-
Health and demographic surveillance systems: a step towards full civil registration and vital statistics system in sub-Sahara Africa?BMC Public Health. 2012 Sep 5;12:741. doi: 10.1186/1471-2458-12-741. BMC Public Health. 2012. PMID: 22950896 Free PMC article.
-
Point-of-contact interactive record linkage (PIRL) between demographic surveillance and health facility data in rural Tanzania.Int J Popul Data Sci. 2017 Sep 18;2(1):3. doi: 10.23889/ijpds.v2i1.408. Epub 2017 Dec 15. Int J Popul Data Sci. 2017. PMID: 30613799 Free PMC article.
-
Health and demographic surveillance systems in low- and middle-income countries: history, state of the art and future prospects.Glob Health Action. 2021 Oct 26;14(sup1):1974676. doi: 10.1080/16549716.2021.1974676. Glob Health Action. 2021. PMID: 35377288 Free PMC article. Review.
-
A Review of Fingerprint Sensors: Mechanism, Characteristics, and Applications.Micromachines (Basel). 2023 Jun 14;14(6):1253. doi: 10.3390/mi14061253. Micromachines (Basel). 2023. PMID: 37374839 Free PMC article. Review.
Cited by
-
Demographic patterns and trends in Central Ghana: baseline indicators from the Kintampo Health and Demographic Surveillance System.Glob Health Action. 2012 Dec 20;5:1-11. doi: 10.3402/gha.v5i0.19033. Glob Health Action. 2012. PMID: 23273249 Free PMC article.
-
The application of a biometric identification technique for linking community and hospital data in rural Ghana.Glob Health Action. 2016 Mar 17;9:29854. doi: 10.3402/gha.v9.29854. eCollection 2016. Glob Health Action. 2016. PMID: 26993473 Free PMC article.
-
The promise of record linkage for assessing the uptake of health services in resource constrained settings: a pilot study from South Africa.BMC Med Res Methodol. 2014 May 24;14:71. doi: 10.1186/1471-2288-14-71. BMC Med Res Methodol. 2014. PMID: 24884457 Free PMC article.
-
Implementation of an electronic fingerprint-linked data collection system: a feasibility and acceptability study among Zambian female sex workers.Global Health. 2015 Jun 27;11:27. doi: 10.1186/s12992-015-0114-z. Global Health. 2015. PMID: 26115656 Free PMC article.
-
Acceptability of Interventions to Improve Engagement in HIV Care Among Pregnant and Postpartum Women at Two Urban Clinics in South Africa.Matern Child Health J. 2019 Sep;23(9):1260-1270. doi: 10.1007/s10995-019-02766-9. Matern Child Health J. 2019. PMID: 31218606 Free PMC article.
References
-
- INDEPTH Network. Population, health and survival at INDEPTH sites. Vol. 1. Ottawa: International Development Research Centre; 2002. Population and health in developing countries.
-
- Sankoh O, Binka F. INDEPTH Network: generating empirical population and health data in resource-constrained countries in the developing world. In: Becher H, Kouyaté B, editors. Health research in developing countries: a collaboration between Burkina Faso and Germany. Berlin: Springer; 2005. pp. 21–32.
-
- INDEPTH Network. Measuring health equity in small areas: findings from demographic surveillance systems. Aldershot, UK and Burlington, VT: Ashgate; 2005.
-
- Adazu K, Lindblade KA, Rosen DH, Odhiambo F, Ofware P, Kwach J, et al. Health and demographic surveillance in rural western Kenya: a platform for evaluating interventions to reduce morbidity and mortality from infectious diseases. Am J Trop Med Hyg. 2005;73:1151–8. - PubMed
-
- Tanser F, Gijsbertsen B, Herbst K. Modelling and understanding primary health care accessibility and utilization in rural South Africa: an exploration using a geographical information system. Soc Sci Med. 2006;63:691–705. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources