

Cell-based immunotherapy with mesenchymal stem cells cures bisphosphonate-related osteonecrosis of the jaw-like disease in mice
- PMID: 20200952
- PMCID: PMC3154005
- DOI: 10.1002/jbmr.37
Cell-based immunotherapy with mesenchymal stem cells cures bisphosphonate-related osteonecrosis of the jaw-like disease in mice
Abstract
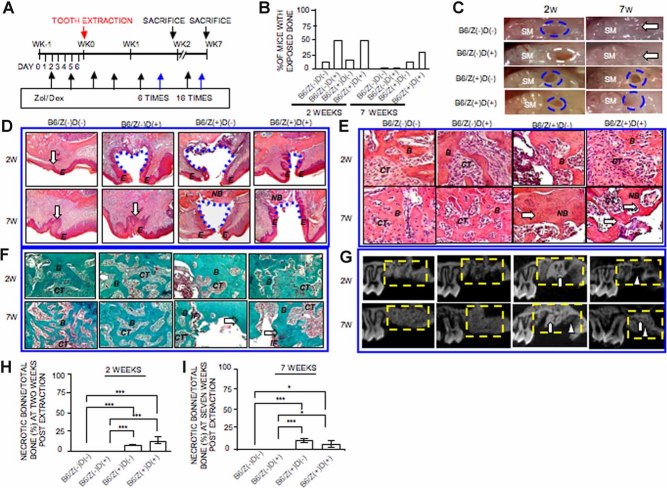
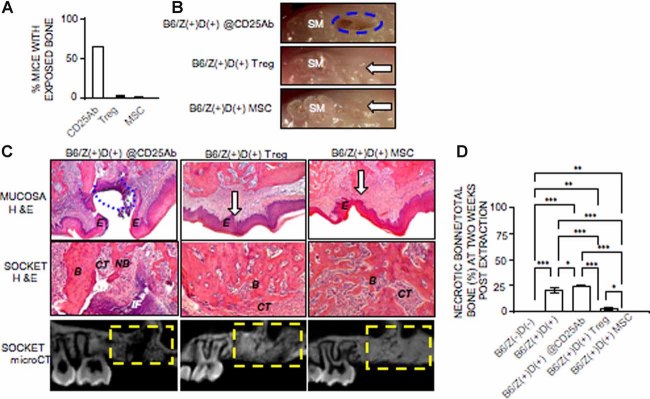
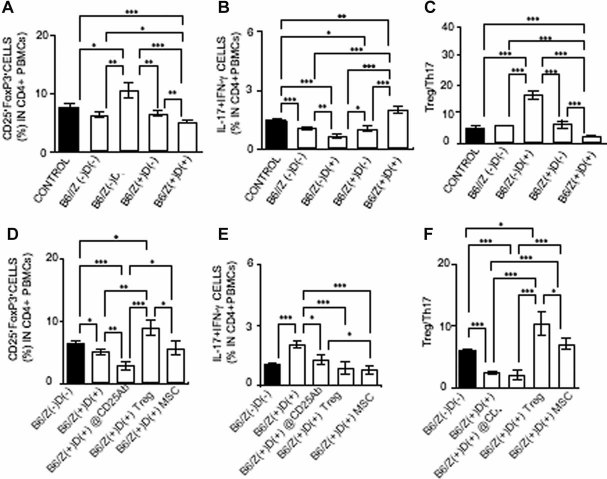
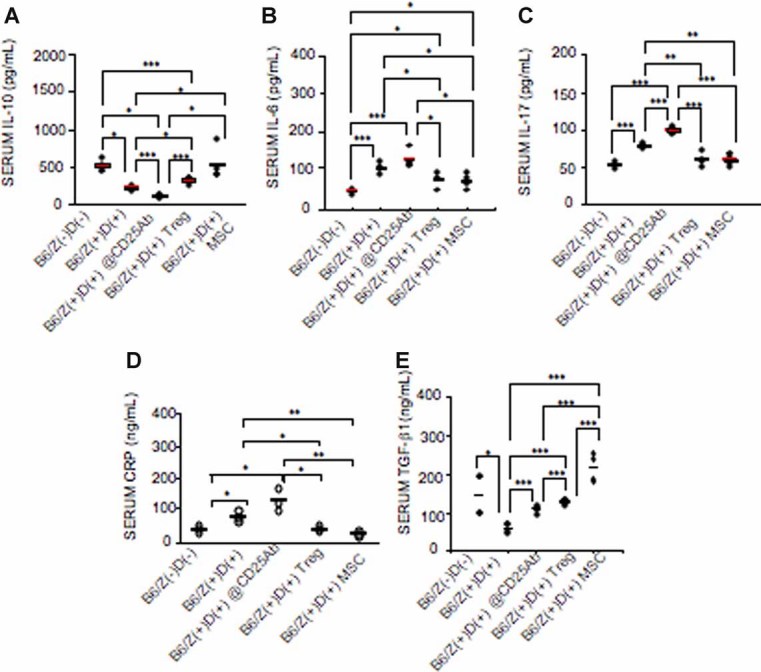
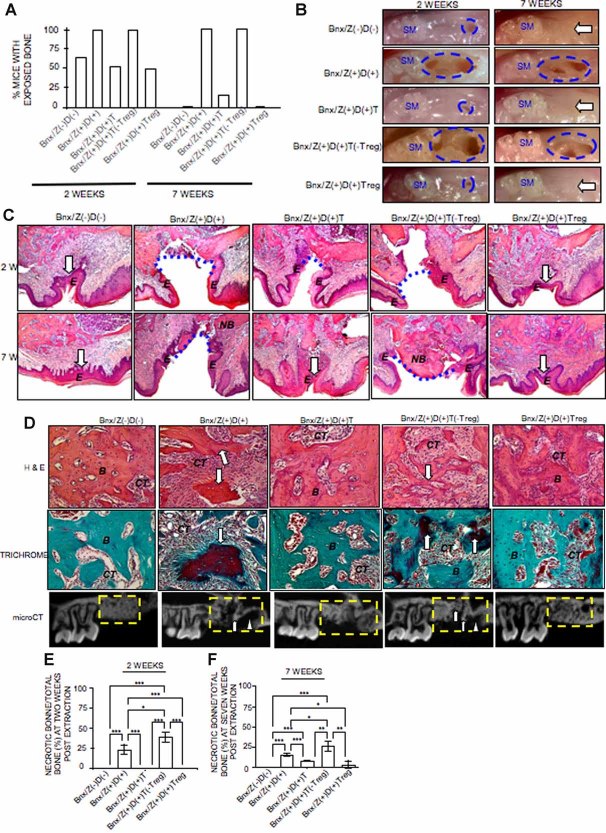
Patients on high-dose bisphosphonate and immunosuppressive therapy have an increased risk of bisphosphonate-related osteonecrosis of the jaw (BRONJ); despite the disease severity, its pathophysiology remains unknown, and appropriate therapy is not established. Here we have developed a mouse model of BRONJ-like disease that recapitulates major clinical and radiographic manifestations of the human disease, including characteristic features of an open alveolar socket, exposed necrotic bone or sequestra, increased inflammatory infiltrates, osseous sclerosis, and radiopaque alveolar bone. We show that administration of zoledronate, a potent aminobisphosphonate, and dexamethasone, an immunosuppressant drug, causes BRONJ-like disease in mice in part by suppressing the adaptive regulatory T cells, Tregs, and activating the inflammatory T-helper-producing interleukin 17 cells, Th17. Most interestingly, we demonstrate that systemic infusion with mesenchymal stem cells (MSCs) prevents and cures BRONJ-like disease possibly via induction of peripheral tolerance, shown as an inhibition of Th17 and increase in Treg cells. The suppressed Tregs/Th17 ratio in zoledronate- and dexamethasone-treated mice is restored in mice undergoing salvage therapy with Tregs. These findings provide evidence of an immunity-based mechanism of BRONJ-like disease and support the rationale for in vivo immunomodulatory therapy using Tregs or MSCs to treat BRONJ.
2010 American Society for Bone and Mineral Research.
Figures
References
-
- Lipton A. New therapeutic agents for the treatment of bone diseases. Expert Opin Biol Ther. 2006;5:817–832. - PubMed
-
- Berenson JR, Hillner BE, Kyle RA, et al. American Society of Clinical Oncology clinical practice guidelines: the role of bisphosphonates in multiple myeloma. J Clin Oncol. 2002;20:3719–3736. - PubMed
-
- Lipton A, Theriault RL, Hortobagyi GN, et al. Pamidronate prevents skeletal complications and is effective palliative treatment in women with breast carcinoma and osteolytic bone metastases: long-term follow-up of two randomized, placebo-controlled trials. Cancer. 2000;88:1082–1090. - PubMed
-
- Berenson JR, Rosen LS, Howell A, et al. Zoledronic acid reduces skeletal-related events in patients with osteolytic metastases. Cancer. 2001;91:1191–1200. - PubMed
-
- Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg. 2003;61:1115–1117. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
