

High treatment failure and default rates for patients with multidrug-resistant tuberculosis in KwaZulu-Natal, South Africa, 2000-2003
- PMID: 20202298
- PMCID: PMC3005763
High treatment failure and default rates for patients with multidrug-resistant tuberculosis in KwaZulu-Natal, South Africa, 2000-2003
Abstract
Setting: Multidrug-resistant tuberculosis (MDR-TB) has emerged as a significant public health threat in South Africa.
Objective: To describe treatment outcomes and determine risk factors associated with unfavorable outcomes among MDR-TB patients admitted to the provincial TB referral hospital in KwaZulu-Natal Province, South Africa.
Design: Retrospective observational study of MDR-TB patients admitted from 2000 to 2003.
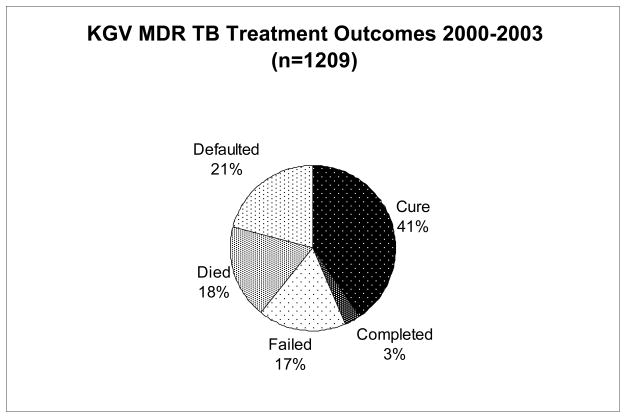
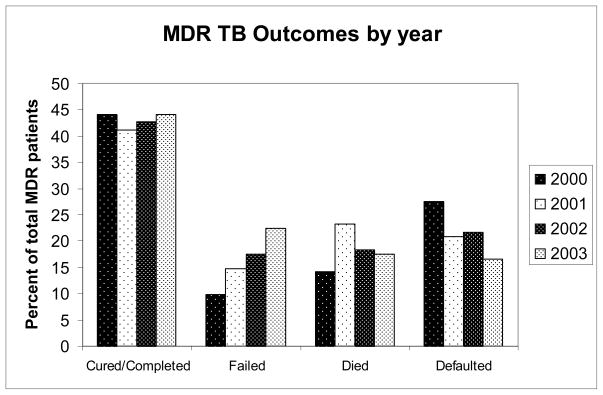
Results: Of 1209 MDR-TB patients with documented treatment outcomes, 491 (41%) were cured, 35 (3%) completed treatment, 208 (17%) failed treatment, 223 (18%) died and 252 (21%) defaulted. Of the total number of patients with known human immunodeficiency virus (HIV) status, 52% were HIV-infected. Treatment failure, death and default each differed in their risk factors. Greater baseline resistance (aOR 2.3-3.0), prior TB (aOR 1.7), and diagnosis in 2001, 2002 or 2003 (aOR 1.9-2.3) were independent risk factors for treatment failure. HIV co-infection was a risk factor for death (aOR 5.6), and both HIV (aOR 2.0) and male sex (aOR 1.9) were risk factors for treatment default.
Conclusion: MDR-TB treatment outcomes in KwaZulu-Natal were substantially worse than those published from other MDR-TB cohorts. Interventions such as concurrent antiretroviral therapy and decentralized MDR-TB treatment should be considered to improve MDR-TB outcomes in this high HIV prevalence setting.
Figures
References
-
- Anti-tuberculosis drug resistance in the world – Report No. 4, The WHO/IUATLD global project on anti-tuberculosis drug resistance surveillance. World Health Organization; Geneva: 2008.
-
- WHO. Global Tuberculosis Control 2008: Surveillance, Planning, Financing. World Health Organization; Geneva: 2008.
-
- Buthelezi SSS. Situational Analysis of TB Drug Resistance in KwaZulu-Natal Province: Republic of South Africa. 2nd Meeting of the Global XDR TB Task Force; Geneva, Switzerland. April 9, 2008.
-
- Weyer K, Lancaster J, Brand J, Van der Waltm MJL Medical Research Council of South Africa. Technical report to the Department of Health. Jun, 2003. Survey of tuberculous drug resistance in South Africa, 2001–2002.
-
- Gandhi NR, Moll A, Sturm AW, et al. Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet. 2006;368:1575–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
