

Disparate evolution of right and left atrial rate during ablation of long-lasting persistent atrial fibrillation
- PMID: 20202517
- PMCID: PMC2892623
- DOI: 10.1016/j.jacc.2009.09.060
Disparate evolution of right and left atrial rate during ablation of long-lasting persistent atrial fibrillation
Abstract
Objectives: The purpose of this study was to assess whether additional ablation in the right atrium (RA) improves termination rate in long-lasting persistent atrial fibrillation (PsAF).
Background: Prolongation of atrial fibrillation (AF) cycle length (CL) measured from the left atrial appendage predicts favorable outcome during catheter ablation of PsAF. However, in some patients, despite prolongation of AF CL in the left atrium (LA) with ablation, AF persists. We hypothesized that this persistence is due to RA drivers, and that these patients may benefit from RA ablation.
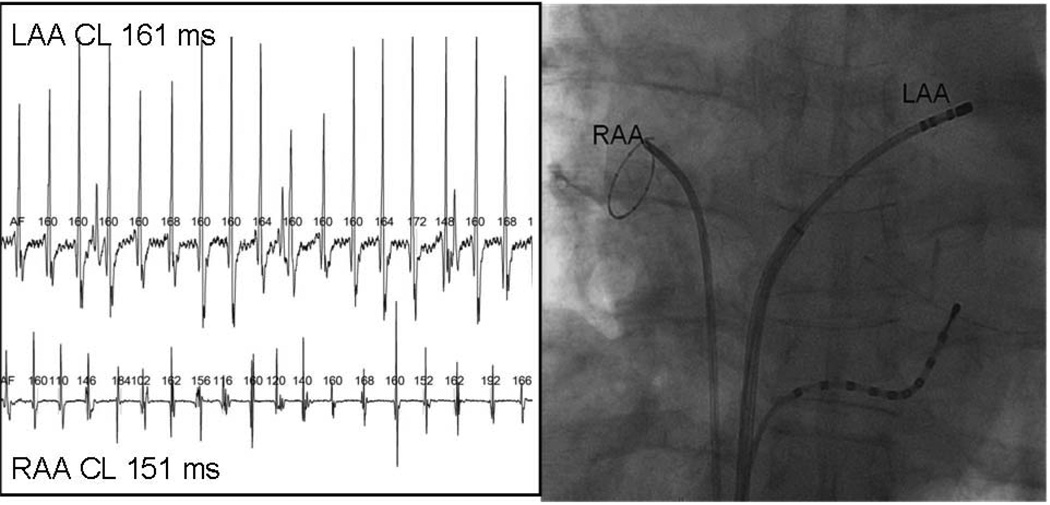
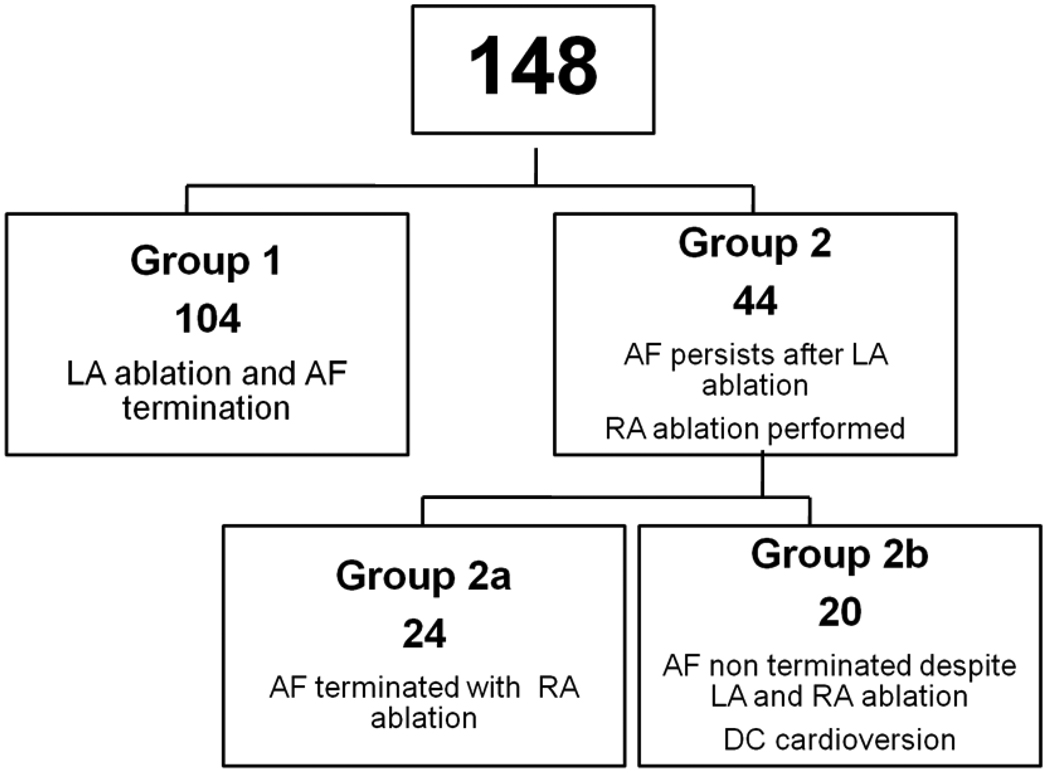
Methods: In all, 148 consecutive patients undergoing catheter ablation of PsAF (duration 25 +/- 32 months) were studied. AF CL was monitored in both atria during stepwise ablation commencing in the LA. Ablation was performed in the RA when all LA sources in AF had been ablated and an RA-LA gradient existed. The procedural end point was AF termination.
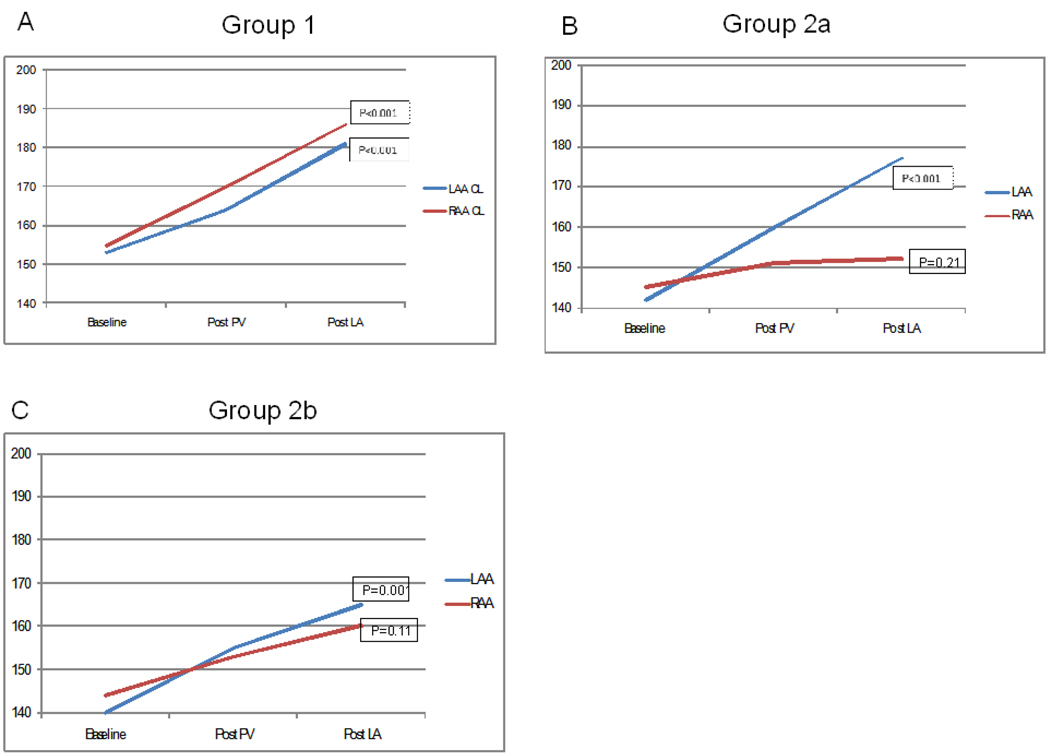
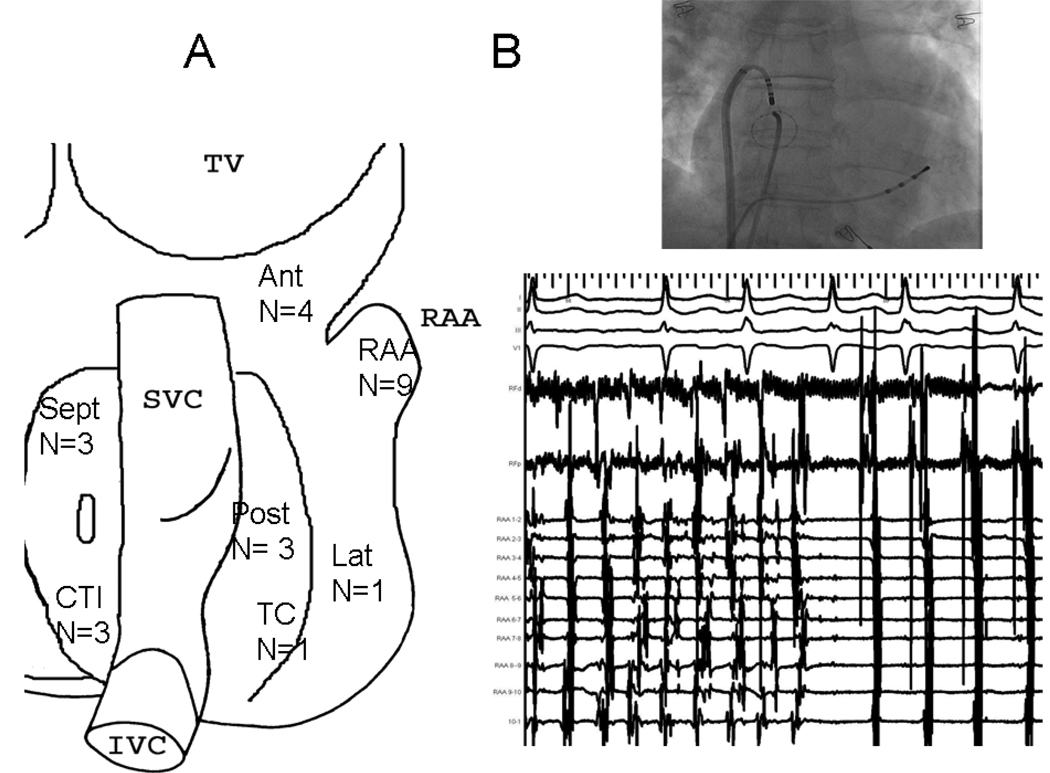
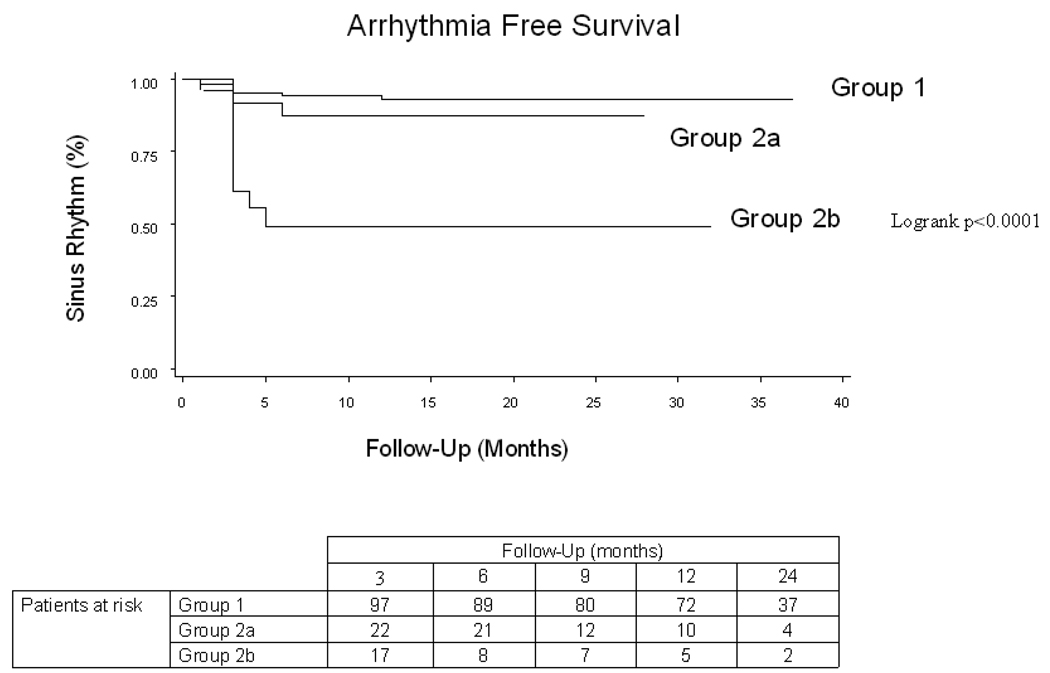
Results: Two distinct patterns of AF CL change emerged during LA ablation. In 104 patients (70%), there was parallel increase of AF CL in LA and RA culminating in AF termination (baseline: LA 153 ms [range 140 to 170 ms], RA 155 ms [range 143 to 171 ms]; after ablation: LA 181 ms [range 170 to 200 ms], RA 186 ms [range 175 to 202 ms]). In 24 patients (19%), RA AF CL did not prolong, creating a right-to-left frequency gradient (baseline: LA 142 ms [range 143 to 153 ms], RA 145 ms [range 139 to 162 ms]; after ablation: LA 177 ms [range 165 to 185 ms], RA 152 ms [range 147 to 175 ms]). These patients had a longer AF history (23 months vs. 12 months, p = 0.001), and larger RA diameter (42 mm vs. 39 mm, p = 0.005), and RA ablation terminated AF in 55%. In the remaining 20 patients, biatrial ablation failed to terminate AF.
Conclusions: A divergent pattern of AF CL prolongation after LA ablation resulted in a right-to-left gradient, demonstrating that the right atrium is driving AF in approximately 20% of PsAF.
Copyright (c) 2010 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Nademanee K, McKenzie J, Kosar E, et al. A new approach for catheter ablation of atrial fibrillation: mapping of the electrophysiologic substrate. J Am Coll Cardiol. 2004;43:2044–2053. - PubMed
-
- Haissaguerre M, Sanders P, Hocini M, et al. Catheter ablation of long-lasting persistent atrial fibrillation: critical structures for termination. J Cardiovasc Electrophysiol. 2005;16:1125–1137. - PubMed
-
- Haissaguerre M, Hocini M, Sanders P, et al. Catheter ablation of long-lasting persistent atrial fibrillation: clinical outcome and mechanisms of subsequent arrhythmias. J Cardiovasc Electrophysiol. 2005;16:1138–1147. - PubMed
-
- Rostock T, Rotter M, Sanders P, et al. High-density activation mapping of fractionated electrograms in the atria of patients with paroxysmal atrial fibrillation. Heart Rhythm. 2006;3:27–34. - PubMed
-
- Oral H, Pappone C, Chugh A, et al. Circumferential pulmonary-vein ablation for chronic atrial fibrillation. N Engl J Med. 2006;354:934–941. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
