

Predicting heart failure hospitalization and mortality by quantitative echocardiography: is body surface area the indexing method of choice? The Heart and Soul Study
- PMID: 20202792
- PMCID: PMC2886012
- DOI: 10.1016/j.echo.2010.01.019
Predicting heart failure hospitalization and mortality by quantitative echocardiography: is body surface area the indexing method of choice? The Heart and Soul Study
Abstract
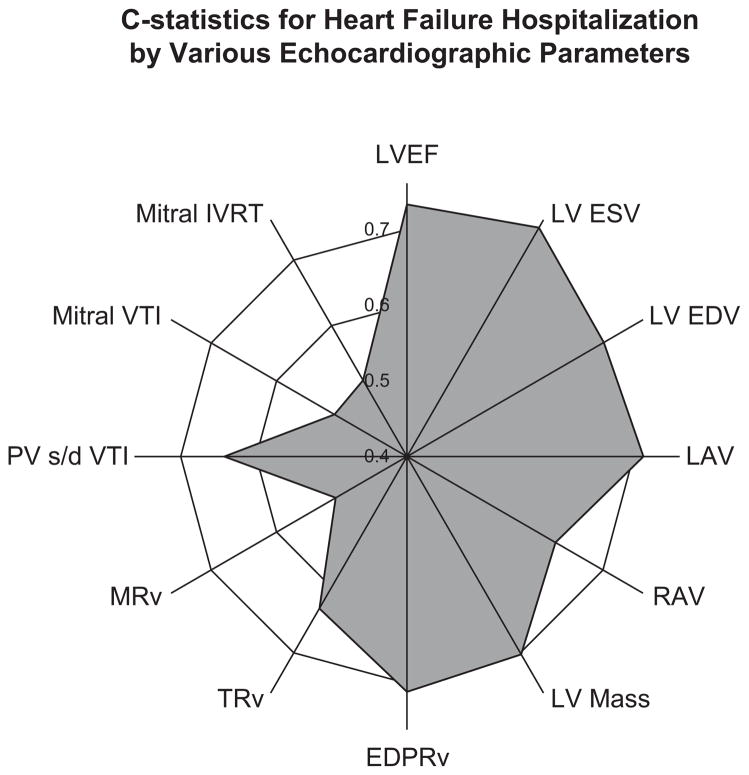
Background: Echocardiographic measurements of left ventricular (LV) mass, left atrial (LA) volume, and LV end-systolic volume (ESV) predict heart failure (HF) hospitalization and mortality. Indexing measurements by body size is thought to establish limits of normality among individuals varying in body habitus. The American Society of Echocardiography recommends dividing measurements by body surface area (BSA), but others have advocated alternative indexing methods.
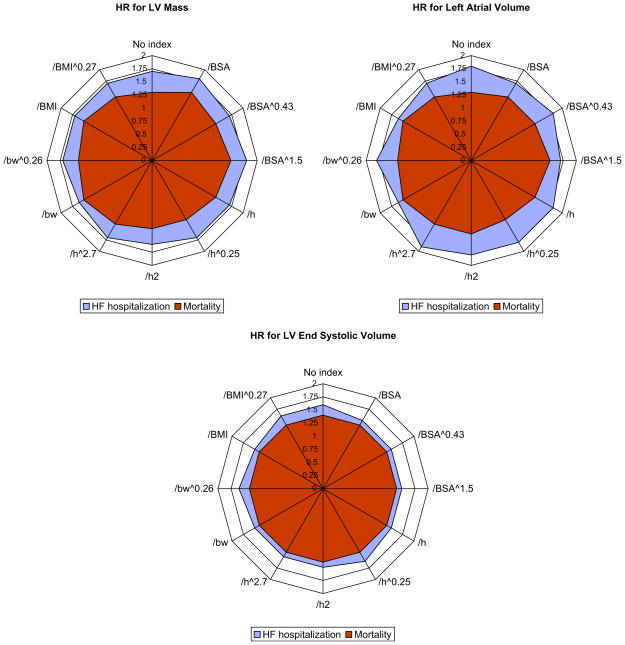
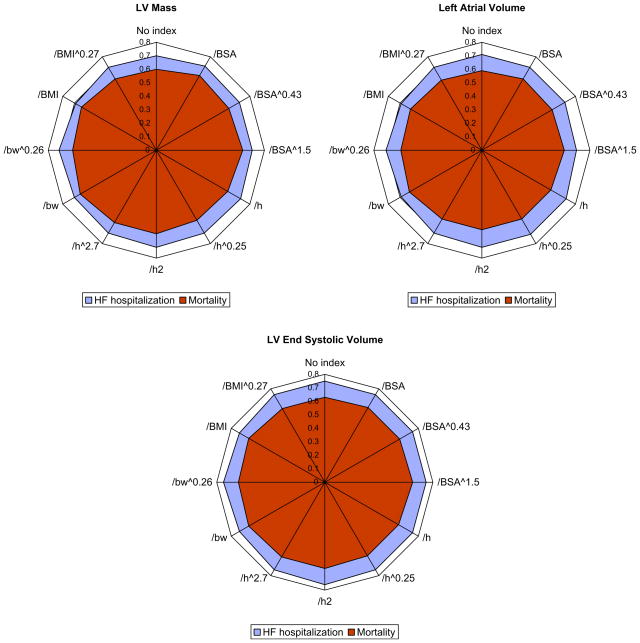
Methods: Echocardiographic measurements were collected in 1024 ambulatory adults with coronary artery disease. LV mass, LA volume, and LV ESV were calculated using truncated ellipse method and biplane method of disk formulae. Comparison between raw measurements and measurements divided by indexing parameters was made by hazard ratios per standard deviation increase in variable and c-statistics for BSA, BSA(0.43), BSA(1.5), height, height(0.25), height(2), height(2.7), body weight (BW), BW(0.26), body mass index (BMI), and BMI(0.27).
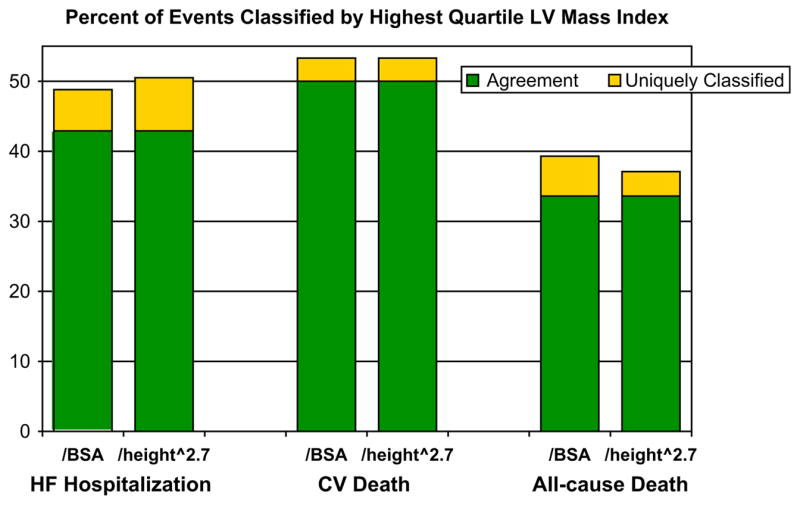
Results: Mean LV mass was 192 +/- 57 g, mean LA volume was 65 +/- 24 mL, and mean LV ESV was 41 +/- 26 mL. Average height was 171 +/- 9 cm, average BSA was 1.94 +/- 0.22 m(2), and average BMI was 28.4 +/- 5.3 kg/m(2). At an average follow-up of 5.6 +/- 1.8 years, there were 148 HF hospitalizations, 71 cardiovascular (CV) deaths, and 269 all-cause deaths. There was excellent correlation between raw measurements and those indexed by height (r = 0.98-0.99), and moderate correlation between raw measurements and those indexed by BW (r = 0.73-0.94). C-statistics and hazard ratios per standard deviation increase in indexed variables were similar for HF hospitalization, CV mortality, and all-cause mortality. There were no significant differences among indexing methods in ability to predict outcomes.
Conclusion: The choice of indexing method by parameters of BSA, height, BW, and BMI does not affect the clinical usefulness of LV mass, LA volume, and LV ESV in predicting HF hospitalization, CV mortality, or all-cause mortality among ambulatory adults with coronary artery disease. Continued use of BSA to index measurements of LV mass, LA volume, and LV ESV is acceptable.
Copyright 2010 American Society of Echocardiography. All rights reserved.
Conflict of interest statement
There are no conflicts of interest to report from any of the authors.
Figures
Comment in
-
Echocardiography: an important tool for cardiovascular risk assessment.J Am Soc Echocardiogr. 2010 Apr;23(4):414-5. doi: 10.1016/j.echo.2010.02.012. J Am Soc Echocardiogr. 2010. PMID: 20362930 No abstract available.
References
-
- Cooper RS, Simmons BE, Castaner A, Santhanam V, Ghali J, Mar M. Left ventricular hypertrophy is associated with worse survival independent of ventricular function and number of coronary arteries severely narrowed. Am J Cardiol. 1990;65:441–5. - PubMed
-
- Benjamin EJ, D’Agostino RB, Belanger AJ, Wolf PA, Levy D. Left atrial size and the risk of stroke and death. The Framingham Heart Study. Circulation. 1995;92:835–41. - PubMed
-
- Kizer JR, Bella JN, Palmieri V, Liu JE, Best LG, Lee ET, et al. Left atrial diameter as an independent predictor of first clinical cardiovascular events in middle-aged and elderly adults: the Strong Heart Study (SHS) Am Heart J. 2006;151:412–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
