

Pregnancy-associated hemolytic uremic syndrome revisited in the era of complement gene mutations
- PMID: 20203157
- PMCID: PMC2865741
- DOI: 10.1681/ASN.2009070706
Pregnancy-associated hemolytic uremic syndrome revisited in the era of complement gene mutations
Abstract
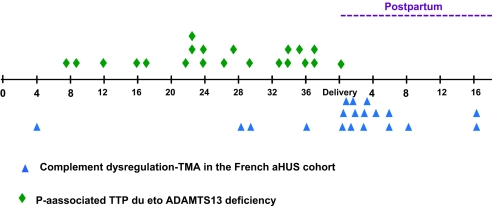
In contrast to pregnancy-associated thrombotic thrombocytopenic purpura, the pathogenesis and presentation of pregnancy-associated atypical hemolytic uremic syndrome (P-aHUS) remain ill-defined. We conducted a retrospective study to assess the presentation and outcomes of patients presenting with P-aHUS and the prevalence of alternative C3 convertase dysregulation. P-aHUS occurred in 21 of the 100 adult female patients with atypical HUS, with 79% presenting postpartum. We detected complement abnormalities in 18 of the 21 patients. The outcomes were poor: 62% reached ESRD by 1 month and 76% by last follow-up. The risk for P-aHUS was highest during a second pregnancy. Thirty-five women, 26 (74%) of whom had complement abnormalities, had at least one pregnancy before the onset of a non-pregnancy-related aHUS. Outcomes did not differ between patients with pregnancy-related and non-pregnancy-related aHUS. Mutations in the SCR19-20 domains of factor H were less frequent in P-aHUS patients compared with non-pregnancy-related aHUS. Pregnancies in female patients with complement abnormalities (n = 44) were complicated by fetal loss and preeclampsia in 4.8% and 7.7%, respectively. Better understanding of complement dysregulation in pregnancy complications is essential, especially to guide development of pharmacologic agents to modulate this system.
Figures


Comment in
-
Pulling the trigger in atypical hemolytic uremic syndrome: the role of pregnancy.J Am Soc Nephrol. 2010 May;21(5):731-2. doi: 10.1681/ASN.2010030308. Epub 2010 Apr 15. J Am Soc Nephrol. 2010. PMID: 20395375 No abstract available.
References
-
- Dashe JS, Ramin SM, Cunningham FG: The long-term consequences of thrombotic microangiopathy (thrombotic thrombocytopenic purpura and hemolytic uremic syndrome) in pregnancy. Obstet Gynecol 91: 662–668, 1998. - PubMed
-
- Furlan M, Robles R, Galbusera M: von Willebrand factor-cleaving protease in thrombotic thrombocytopenic purpura and the hemolytic-uremic syndrome. N Engl J Med 339: 1578–1584, 1998. - PubMed
-
- Levy GG, Nichols WC, Lian EC: Mutations in a member of the ADAMTS gene family cause thrombotic thrombocytopenic purpura. Nature 413: 488–494, 2001. - PubMed
-
- Walport MJ: Complement. First of two parts. N Engl J Med 344: 1058–1066, 2001. - PubMed
-
- Noris M, Remuzzi G. Atypical hemolytic-uremic syndrome. N Engl J Med 361: 1676–1687, 200911 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
