

Serum potassium and outcomes in CKD: insights from the RRI-CKD cohort study
- PMID: 20203167
- PMCID: PMC2863985
- DOI: 10.2215/CJN.05850809
Serum potassium and outcomes in CKD: insights from the RRI-CKD cohort study
Abstract
Background and objectives: The relationship between serum potassium (S(K)) and mortality in chronic kidney disease (CKD) has not been systematically investigated.
Design, setting, participants, & measurements: We examined the predictors and mortality association of S(K) in the Renal Research Institute CKD Study cohort, wherein 820 patients with CKD were prospectively followed at four US centers for an average of 2.6 years. Predictors of S(K) were investigated using linear and repeated measures regression models. Associations between S(K) and mortality, the outcomes of ESRD, and cardiovascular events in time-dependent Cox models were examined.
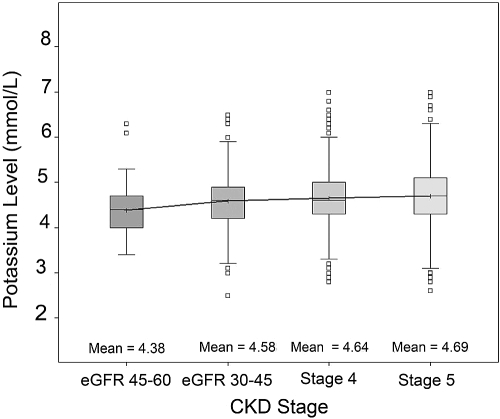
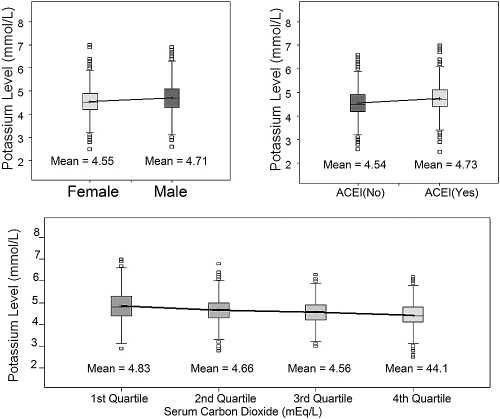
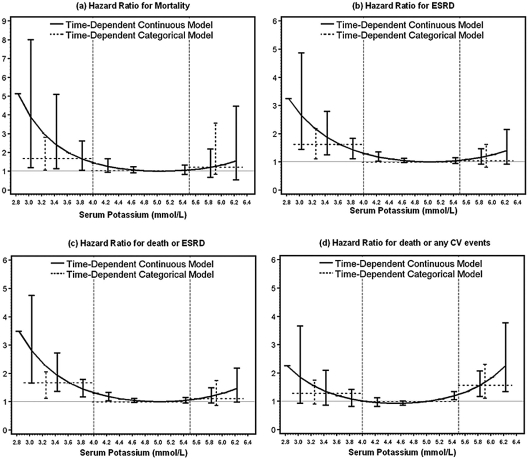
Results: The mean age was 60.5 years, 80% were white, 90% had hypertension, 36% had diabetes, the average estimated GFR was 25.4 ml/min per 1.73 m(2), and mean baseline S(K) was 4.6 mmol/L. Higher S(K) was associated with male gender, lower estimated GFR and serum bicarbonate, absence of diuretic and calcium channel blocker use, diabetes, and use of angiotensin-converting enzyme inhibitors and/or statins. A U-shaped relationship between S(K) and mortality was observed, with mortality risk significantly greater at S(K) < or = 4.0 mmol/L compared with 4.0 to 5.5 mmol/L. Risk for ESRD was elevated at S(K) < or = 4 mmol/L in S(K) categorical models. Only the composite of cardiovascular events or death as an outcome was associated with higher S(K) (> or = 5.5).
Conclusions: Although clinical practice usually emphasizes greater attention to elevated S(K) in the setting of CKD, our results suggest that patients who have CKD and low or even low-normal S(K) are at higher risk for dying than those with mild to moderate hyperkalemia.
Figures
References
-
- Tzamaloukas AH, Avasthi PS: Temporal profile of serum potassium concentration in nondiabetic and diabetic outpatients on chronic dialysis. American J Nephrol 7: 101– 109, 1987 - PubMed
-
- Sacchetti A, Stuccio N, Panebianco P, Torres M: ED hemodialysis for treatment of renal failure emergencies. Am J Emerg Med 17: 305– 307, 1999 - PubMed
-
- Morduchowicz G, Winkler J, Derazne E, Van Dyk DJ, Wittenberg C, Zabludowski JR, Shohat J, Rosenfeld JB, Boner G: Causes of death in patients with end-stage renal disease treated by dialysis in a center in Israel. Isr J Med Sci 28: 776– 779, 1992 - PubMed
-
- Shibata M, Kishi T, Iwata H: Clinical study of complications in dialyzed diabetics. Tohoku J Exp Med 141[ Suppl]: 417– 425, 1983 - PubMed
-
- Stevens MS, Dunlay RW: Hyperkalemia in hospitalized patients. Int Urol Nephrol 32: 177– 180, 2000 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
