

Review
doi: 10.1038/ajg.2009.728.
Pathology of gastric intestinal metaplasia: clinical implications
Affiliations
- PMID: 20203636
- PMCID: PMC2895407
- DOI: 10.1038/ajg.2009.728
Item in Clipboard
Review
Pathology of gastric intestinal metaplasia: clinical implications
Am J Gastroenterol.
2010 Mar.
No abstract available
Conflict of interest statement
Figures
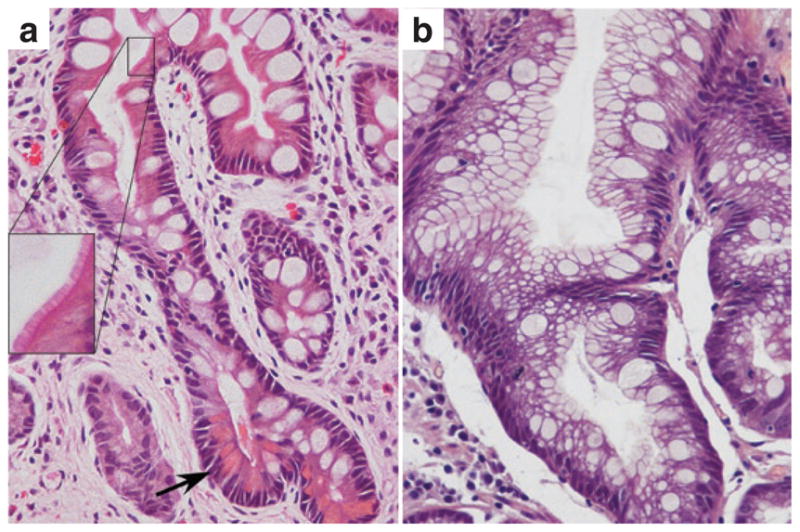
Photomicrographs of gastric intestinal metaplasia. (a) Complete type with well-defined goblet cells alternating with eosinophilic enterocytes displaying well-developed brush border (inset) and Paneth cells (arrow). (b) Incomplete type showing multiple intracytoplasmic mucin droplets of varying sizes and shapes, and absence of a brush border. (Hematoxylin and eosin; original magnification, ×400; inset, ×1,000.)
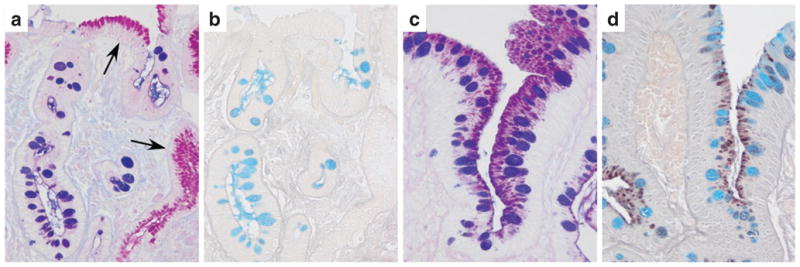
Histochemical staining of gastric intestinal metaplasia (IM). (a, c) Periodic acid–Schiff–Alcian blue staining. Neutral mucins are stained magenta (arrows show normal epithelium), and acid mucins are blue (or purple when combined with neutral). (b, d) Alcian blue–high-iron diamine technique differentiates acid mucins. Sialomucins are stained blue, and sulfomucins are brown. (a, b) Complete IM (type I) shows sialomucins in goblet cells, and absence of sulfomucins. (c, d) Incomplete IM (type III) with sialomucins in goblet cells and a mixture of neutral and sulfomucins in columnar cells. (Original magnification, ×400.)
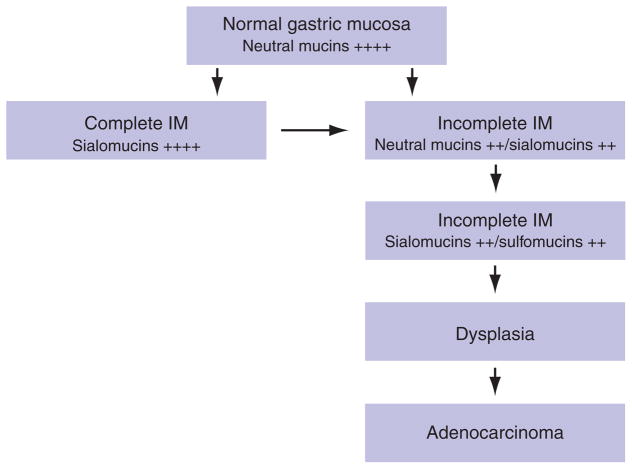
Diagrammatic representation of the sequential steps in intestinal metaplasia (IM), indicating the mucin types expressed in each step. Staining intensities are represented by the symbols + to ++++.
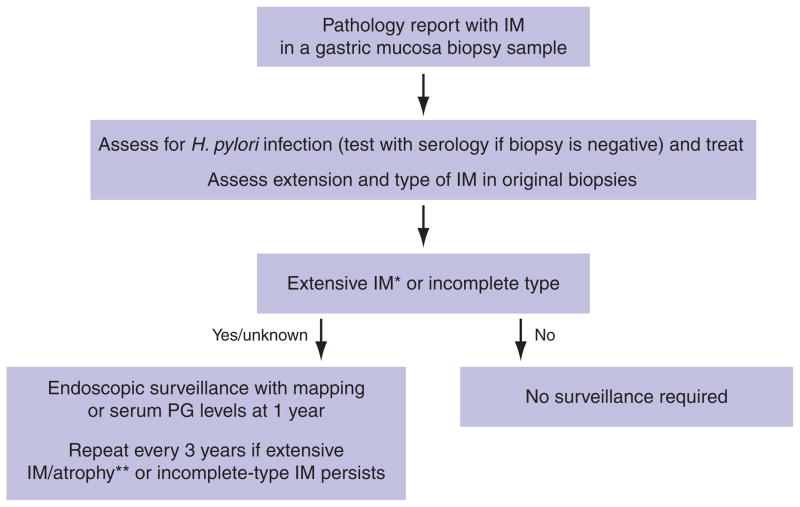
Proposed algorithm for the management and surveillance of gastric intestinal metaplasia (IM). *Definition of extensive IM: (i) IM present in at least two gastric locations or (ii) moderate or marked IM in at least two biopsy specimens (see refs. and 36). **Definition of extensive atrophy: serum pepsinogen I (PGI) level <70 μg/l and PGI/PGII ratio <3.
References
-
- Correa P. Human gastric carcinogenesis: a multistep and multifactorial process. First American Cancer Society Award Lecture on Cancer Epidemiology and Prevention. Cancer Res. 1992;52:6735–40. - PubMed
-
- Fennerty MB. Gastric intestinal metaplasia on routine endoscopic biopsy. Gastroenterology. 2003;125:586–90. - PubMed
-
- Brown LM, Devesa SS. Epidemiologic trends in esophageal and gastric cancer in the United States. Surg Oncol Clin N Am. 2002;11:235–56. - PubMed
-
- Devesa SS, Blot WJ, Fraumeni JF., Jr Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer. 1998;83:2049–53. - PubMed
-
- Goldblum JR, Richter JE, Vaezi M, et al. Helicobacter pylori infection, not gastroesophageal reflux, is the major cause of inflammation and intestinal metaplasia of gastric cardiac mucosa. Am J Gastroenterol. 2002;97:302–11. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
