

Therapy of chronic wounds with water-filtered infrared-A (wIRA)
- PMID: 20204086
- PMCID: PMC2831243
Therapy of chronic wounds with water-filtered infrared-A (wIRA)
Abstract
The central portion of chronic wounds is often hypoxic and relatively hypothermic, representing a deficient energy supply of the tissue, which impedes wound healing or even makes it impossible. Water-filtered infrared-A (wIRA) is a special form of heat radiation with a high tissue penetration and a low thermal load to the skin surface. wIRA produces a therapeutically usable field of heat and increases temperature, oxygen partial pressure and perfusion of the tissue. These three factors are decisive for a sufficient tissue supply with energy and oxygen and consequently as well for wound healing, especially in chronic wounds, and infection defense. wIRA acts both by thermal and thermic as well as by non-thermal and non-thermic effects. wIRA can advance wound healing or improve an impaired wound healing process and can especially enable wound healing in non-healing chronic wounds. wIRA can considerably alleviate the pain and diminish wound exudation and inflammation and can show positive immunomodulatory effects.In a prospective, randomized, controlled study of 40 patients with chronic venous stasis ulcers of the lower legs irradiation with wIRA and visible light (VIS) accelerated the wound healing process (on average 18 vs. 42 days until complete wound closure, residual ulcer area after 42 days 0.4 cm(2) vs. 2.8 cm(2)) and led to a reduction of the required dose of pain medication in comparison to the control group of patients treated with the same standard care (wound cleansing, wound dressing with antibacterial gauze, and compression garment therapy) without the concomitant irradiation. Another prospective study of 10 patients with non-healing chronic venous stasis ulcers of the lower legs included extensive thermographic investigation. Therapy with wIRA(+VIS) resulted in a complete or almost complete wound healing in 7 patients and a marked reduction of the ulcer size in another 2 of the 10 patients, a clear reduction of pain and required dose of pain medication, and a normalization of the thermographic image. In a current prospective, randomized, controlled, blinded study patients with non-healing chronic venous stasis ulcers of the lower legs are treated with compression garment therapy, wound cleansing, wound dressings and 30 minutes irradiation five times per week over 9 weeks. A preliminary analysis of the first 23 patients of this study has shown in the group with wIRA(+VIS) compared to a control group with VIS an advanced wound healing, an improved granulation and in the later phase of treatment a decrease of the bacterial burden. Some case reports have demonstrated that wIRA can also be used for mixed arterial-venous ulcers or arterial ulcers, if irradiation intensity is chosen appropriately low and if irradiation is monitored carefully. wIRA can be used concerning decubital ulcers both in a preventive and in a therapeutic indication. wIRA can improve the resorption of topically applied substances also on wounds. An irradiation with VIS and wIRA presumably acts with endogenous protoporphyrin IX (or protoporphyrin IX of bacteria) virtually similar as a mild photodynamic therapy (endogenous PDT-like effect). This could lead to improved cell regeneration and wound healing and to antibacterial effects. In conclusion, these results indicate that wIRA generally should be considered for the treatment of chronic wounds.
Das Zentrum von chronischen Wunden ist oft hypoxisch und relativ hypotherm. Dies entspricht einer defizitären Energiebereitstellung im Gewebe, die die Wundheilung behindert oder unmöglich macht. Wassergefiltertes Infrarot A (wIRA) ist eine spezielle Form der Wärmestrahlung mit hohem Eindringvermögen in das Gewebe bei geringer thermischer Oberflächenbelastung. wIRA erzeugt ein therapeutisch nutzbares Wärmefeld und steigert Temperatur, Sauerstoffpartialdruck sowie die Durchblutung im Gewebe. Diese drei Faktoren sind entscheidend für eine ausreichende Versorgung des Gewebes mit Energie und Sauerstoff und deshalb auch für die Wundheilung, speziell bei chronischen Wunden, und die Infektionsabwehr. wIRA wirkt sowohl über thermische und temperaturabhängige als auch über nicht-thermische und temperaturunabhängige Effekte. wIRA kann die Wundheilung beschleunigen oder einen stagnierenden Wundheilungsprozess verbessern und insbesondere bei nicht-heilenden chronischen Wunden eine Wundheilung ermöglichen. wIRA vermag Schmerzen deutlich zu mindern und die Wundsekretion sowie Entzündung zu reduzieren sowie positive immunmodulierende Effekte zu zeigen.
In einer prospektiven, randomisierten, kontrollierten Studie mit 40 Patienten mit chronischen venösen Unterschenkelulzera führte eine Bestrahlung mit wIRA und sichtbarem Licht (VIS) zu einer schnelleren Wundheilung (im Durchschnitt 18 vs. 42 Tage bis zum kompletten Wundschluss, Restulkusfläche nach 42 Tagen 0,4 cm² vs. 2,8 cm²) und einem geringeren Schmerzmittelverbrauch gegenüber einer in gleicher Form (Wundsäuberung, antibakterielle Wundauflagen und Kompressionstherapie) therapierten, aber nicht bestrahlten Kontrollgruppe.
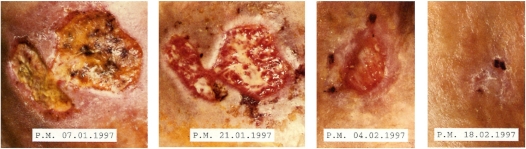
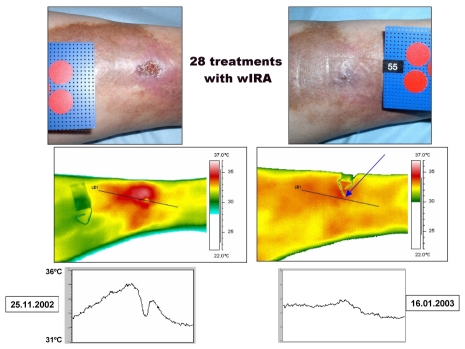
Eine weitere prospektive Studie mit 10 Patienten mit aufwändiger thermographischer Verlaufskontrolle ergab unter Therapie mit wIRA(+VIS) eine vollständige oder fast vollständige Abheilung therapierefraktärer chronischer Unterschenkelulzera bei 7 sowie eine deutliche Ulkusverkleinerung bei 2 weiteren der 10 Patienten, eine ausgeprägte Minderung der Schmerzen und des Schmerzmittelverbrauchs und eine Normalisierung des thermographischen Bildes.
In einer laufenden prospektiven, randomisierten, kontrollierten, verblindeten Studie werden Patienten mit nicht-heilenden chronischen venösen Unterschenkelulzera mit Kompressionstherapie, Wundsäuberung und nicht-adhäsiven Wundauflagen sowie 30 Minuten Bestrahlung fünfmal pro Woche über 9 Wochen behandelt. Eine vorläufige Auswertung der ersten 23 Patienten zeigte, dass die Gruppe mit wIRA(+VIS) verglichen mit einer Kontrollgruppe mit VIS eine schnellere Wundheilung, eine bessere Granulation und in der späteren Phase der Behandlung eine Abnahme der bakteriellen Last der Wunden aufwies.
Einige Fallberichte haben gezeigt, dass wIRA selbst bei gemischt arteriell-venösen Ulzera oder arteriellen Ulzera eingesetzt werden kann, wenn die Bestrahlungsstärke angemessen niedrig gewählt und die Bestrahlung sorgfältig überwacht wird. wIRA kann bei Dekubitalulzera sowohl präventiv als auch therapeutisch eingesetzt werden. wIRA kann die Resorption topisch applizierter Substanzen auch auf Wunden verbessern.
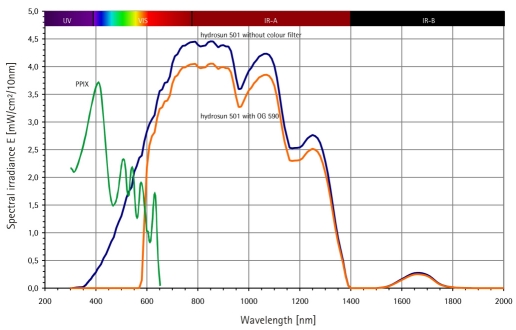
Eine Bestrahlung mit VIS und wIRA wirkt vermutlich in Verbindung mit endogenem Protoporphyrin IX (oder Protoporphyrin IX von Bakterien) quasi ähnlich wie eine milde photodynamische Therapie (endogener PDT-ähnlicher Effekt). Dies kann die Zellregeneration und Wundheilung fördern und antibakteriell wirken.
Zusammengefasst zeigen die Ergebnisse, dass wIRA generell für die Behandlung chronischer Wunden erwogen werden sollte.
Keywords: chronic venous stasis ulcers of the lower legs; chronic wounds; energy supply; infection defense; inflammation; infrared thermography; oxygen supply; problem wounds; prospective, randomized, controlled, blinded study; quality of life; reduction of pain; thermal and non-thermal effects; thermic and non-thermic effects; thermographic image analysis; tissue blood flow; tissue oxygen partial pressure; tissue temperature; visual analog scales (VAS); water-filtered infrared-A (wIRA); wound exudation; wound healing; wound infections.
Figures



Similar articles
-
Heat for wounds - water-filtered infrared-A (wIRA) for wound healing - a review.Ger Med Sci. 2016 Jun 29;14:Doc08. doi: 10.3205/000235. eCollection 2016. Ger Med Sci. 2016. PMID: 27408610 Free PMC article. Review.
-
Improvement of wound healing by water-filtered infrared-A (wIRA) in patients with chronic venous stasis ulcers of the lower legs including evaluation using infrared thermography.Ger Med Sci. 2008 Oct 21;6:Doc11. Ger Med Sci. 2008. PMID: 19675738 Free PMC article.
-
Therapy of acute wounds with water-filtered infrared-A (wIRA).GMS Krankenhhyg Interdiszip. 2007 Dec 28;2(2):Doc53. GMS Krankenhhyg Interdiszip. 2007. PMID: 20204084 Free PMC article.
-
Water-filtered infrared-A (wIRA) in acute and chronic wounds.GMS Krankenhhyg Interdiszip. 2009 Dec 16;4(2):Doc12. doi: 10.3205/dgkh000137. GMS Krankenhhyg Interdiszip. 2009. PMID: 20204090 Free PMC article.
-
[Water-filtered infrared-A (wIRA) promotes wound healing].Chirurg. 2014 Nov;85(11):980-92. doi: 10.1007/s00104-014-2809-8. Chirurg. 2014. PMID: 25385134 Review. German.
Cited by
-
Adjuvant Transgingival Therapy with Visible Light Plus Water-Filtered Infrared-A (VIS + wIRA) in Periodontal Therapy-A Randomized, Controlled, Stratified, Double-Blinded Clinical Trial.Antibiotics (Basel). 2021 Mar 3;10(3):251. doi: 10.3390/antibiotics10030251. Antibiotics (Basel). 2021. PMID: 33802497 Free PMC article.
-
Effect of laser therapy on expression of angio- and fibrogenic factors, and cytokine concentrations during the healing process of human pressure ulcers.Int J Med Sci. 2018 Jul 13;15(11):1105-1112. doi: 10.7150/ijms.25651. eCollection 2018. Int J Med Sci. 2018. PMID: 30123047 Free PMC article. Clinical Trial.
-
Antimicrobial Photoinactivation Using Visible Light Plus Water-Filtered Infrared-A (VIS + wIRA) Alters In Situ Oral Biofilms.PLoS One. 2015 Jul 10;10(7):e0132107. doi: 10.1371/journal.pone.0132107. eCollection 2015. PLoS One. 2015. PMID: 26162100 Free PMC article.
-
Heat for wounds - water-filtered infrared-A (wIRA) for wound healing - a review.Ger Med Sci. 2016 Jun 29;14:Doc08. doi: 10.3205/000235. eCollection 2016. Ger Med Sci. 2016. PMID: 27408610 Free PMC article. Review.
-
[Importance of modern treatment procedures for infected and colonized wounds in dermatology].Hautarzt. 2014 Nov;65(11):949-59. doi: 10.1007/s00105-014-3526-4. Hautarzt. 2014. PMID: 25336295 German.
References
-
- Hoffmann G. Principles and working mechanisms of water-filtered infrared-A (wIRA) in relation to wound healing [review] GMS Krankenhaushyg Interdiszip. 2007;2(2):Doc54. Available from: http://www.egms.de/en/journals/dgkh/2007-2/dgkh000087.shtml. - PMC - PubMed
-
- Hoffmann G. Wassergefiltertes Infrarot A (wIRA) zur Verbesserung der Wundheilung [Übersichtsarbeit] [Water-filtered infrared A (wIRA) for the improvement of wound healing [review]]. GMS Krankenhaushyg Interdiszip. 2006;1(1):Doc20. (Ger). Available from: http://www.egms.de/en/journals/dgkh/2006-1/dgkh000020.shtml.
-
- Hartel M, Illing P, Mercer JB, Lademann J, Daeschlein G, Hoffmann G. Therapy of acute wounds with water-filtered infrared-A (wIRA) [review] GMS Krankenhaushyg Interdiszip. 2007;2(2):Doc53. Available from: http://www.egms.de/en/journals/dgkh/2007-2/dgkh000086.shtml. - PMC - PubMed
-
- Hartel M, Hoffmann G, Wente MN, Martignoni ME, Büchler MW, Friess H. Randomized clinical trial of the influence of local water-filtered infrared A irradiation on wound healing after abdominal surgery. Br J Surg. 2006;93(8):952–960. doi: 10.1002/bjs.5429. Available from: http://dx.doi.org/10.1002/bjs.5429. - DOI - DOI - PubMed
LinkOut - more resources
Full Text Sources