

Tape functionality: position, change in shape, and outcome after TVT procedure--mid-term results
- PMID: 20204326
- PMCID: PMC2876268
- DOI: 10.1007/s00192-010-1119-z
Tape functionality: position, change in shape, and outcome after TVT procedure--mid-term results
Erratum in
- Int Urogynecol J Pelvic Floor Dysfunct. 2010 Nov;21(11):1439-41
Abstract
Introduction and hypothesis: This study evaluates the relevance of the tape position and change in shape (tape functionality) under in vivo conditions for mid-term outcome.
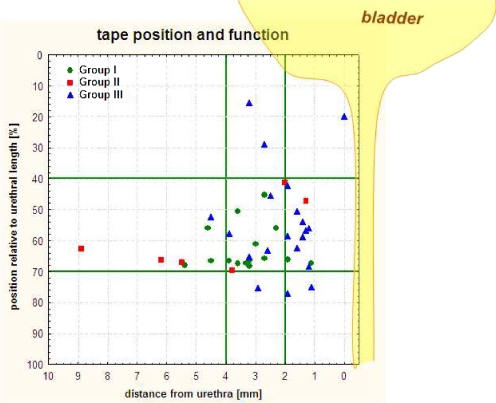
Methods: Changes in the sonographic tension-free vaginal tape (TVT) position relative to the percentage urethral length and the tape-urethra distance were determined after 6 and 48 months in 41 women with stress urinary incontinence.
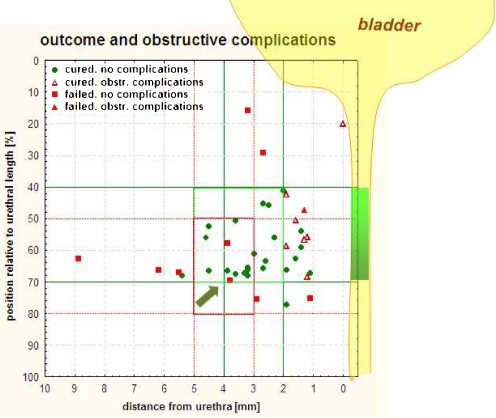
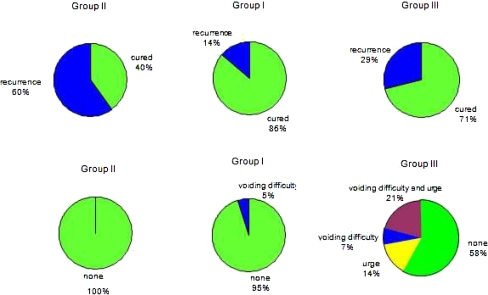
Results: At 48 months, 76% (31/41) of women were cured, 17% (7/41) were improved, and 7% (3/41) were failures. Disturbed bladder voiding was present in 12% (5/41), de novo urge incontinence in 7% (3/41). The median TVT position was at 63% of urethral length. Median tape-urethra distance was 2.7 mm, ranging from 2.9 mm in continent patients without complications to 1.1 mm in those with obstructive complications. Patients with postoperative urine loss had a median distance of 3.9 mm. The tape was stretched at rest and C-shaped during straining in 15 of 41 women (37%) at 48 months (all continent). Patients with this tape functionality at 6 months were also cured at 48 months in 86% of cases (19/22), and only 14% (3/22) showed recurrent incontinence.
Conclusions: Mid-term data suggest an optimal outcome if the tape is positioned at least 2 mm from the urethra at the junction of the middle and distal thirds. Patients with optimal tape functionality at 6 months are likely to show mid-term therapeutic success.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
