

Prevalence of major levator abnormalities in symptomatic patients with an underactive pelvic floor contraction
- PMID: 20204327
- PMCID: PMC2876255
- DOI: 10.1007/s00192-010-1111-7
Prevalence of major levator abnormalities in symptomatic patients with an underactive pelvic floor contraction
Abstract
Introduction and hypothesis: Major levator ani abnormalities (LAA) may lead to abnormal pelvic floor muscle contraction (pfmC) and secondarily to stress urinary incontinence (SUI), prolapse, or fecal incontinence (FI).
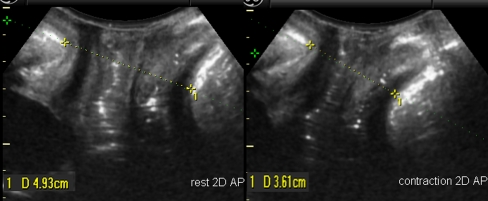
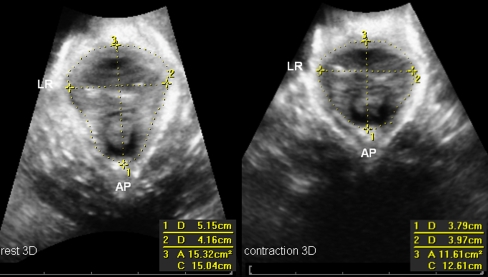
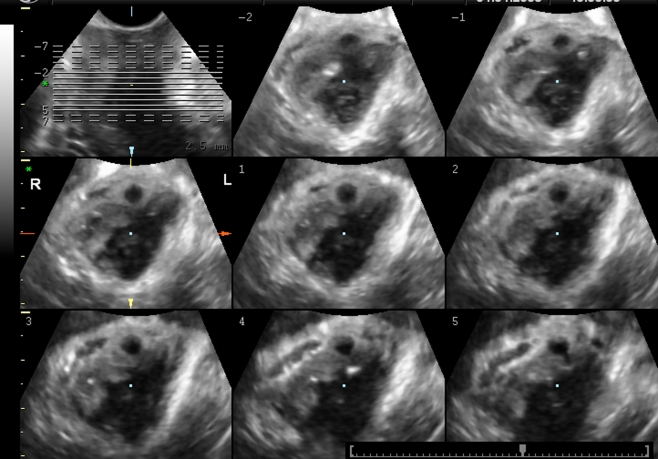
Methods: A retrospective observational study included 352 symptomatic patients to determine prevalence of LAA in underactive pfmC and the relationship with symptoms. On 2D/3D transperineal ultrasound, PfmC was subjectively assessed as underactive (UpfmC) or normal (NpfmC) and quantified. LAA, defined as a complete avulsion of the pubic bone, was analyzed using tomographic ultrasound imaging.
Results: LAA were found in 53.8% of women with UpfmC versus 16.1% in NpfmC (P < 0.001). Patients with UpfmC were less likely to reduce hiatal area on pfmC (mean 7% reduction vs 25% in NpfmC (P < 0.001)). An UpfmC was associated with FI (P = 0.002), not with SUI or prolapse of the anterior and central compartment.
Conclusion: An underactive pfmC is associated with increased prevalence of LAA and FI.
Figures
References
-
- Bo K, Finckenhagen HB. Vaginal palpation of pelvic floor muscle strength: inter-test reproducibility and comparison between palpation and vaginal squeeze pressure. Acta Obstet Gynecol Scand. 2001;80:883–887. - PubMed
-
- Messelink B, Benson T, Berghmans B, Bo K, Corcos J, Fowler C, et al. Standardization of terminology of pelvic floor muscle function and dysfunction: report from the pelvic floor clinical assessment group of the International Continence Society. Neurourol Urodyn. 2005;24:374–380. doi: 10.1002/nau.20144. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
