

Systematic review of D2 lymphadenectomy versus D2 with para-aortic nodal dissection for advanced gastric cancer
- PMID: 20205287
- PMCID: PMC2835793
- DOI: 10.3748/wjg.v16.i9.1138
Systematic review of D2 lymphadenectomy versus D2 with para-aortic nodal dissection for advanced gastric cancer
Abstract
Aim: To evaluate the feasibility and therapeutic effects of para-aortic nodal dissection (PAND) for advanced gastric cancer.
Methods: Randomized controlled trials (RCTs) and non-randomized studies comparing D2 + PAND with D2 lymphadenectomy were identified using a pre-defined search strategy. Five-year overall survival rate, post-operative mortality, and wound degree of surgery between the two operations were compared by using the methods provided by the Cochrane Handbook for Systematic Reviews of Interventions.
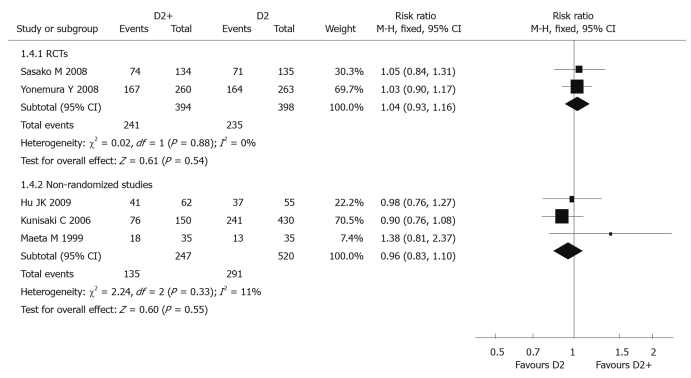
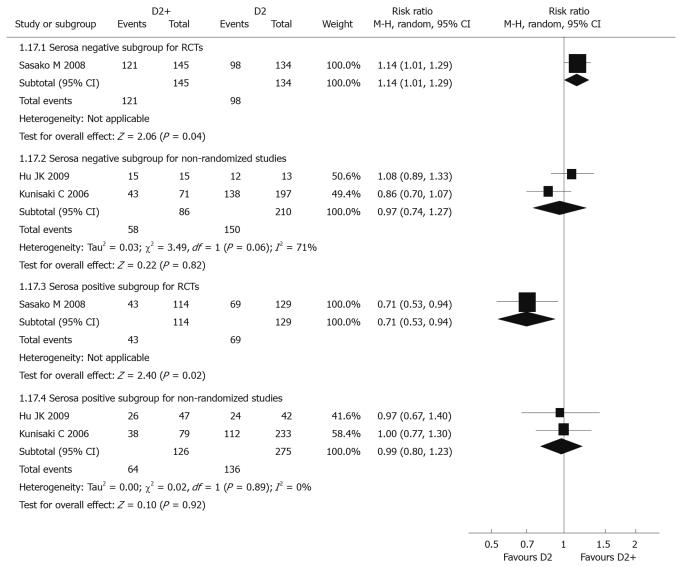
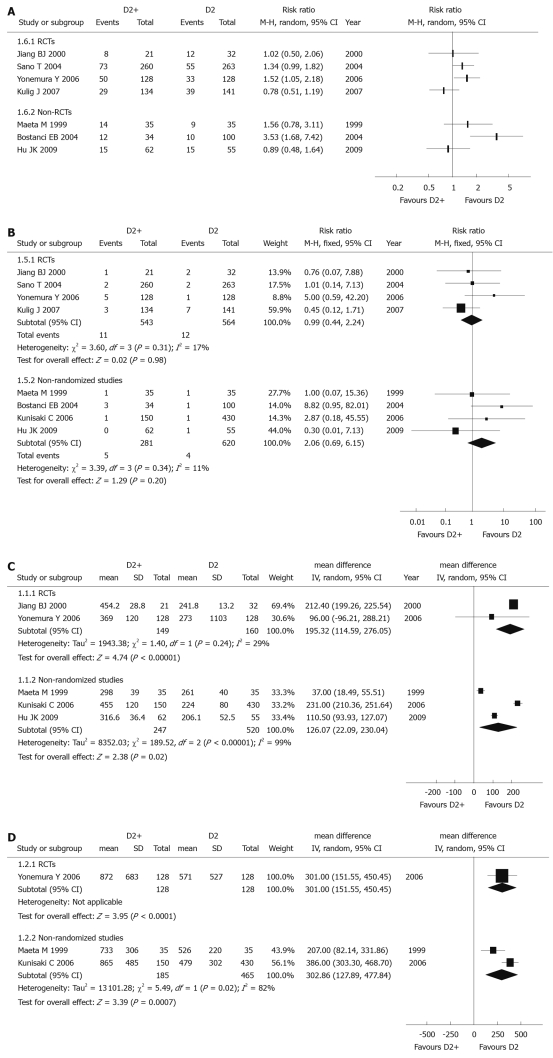
Results: Four RCTs (1120 patients) and 4 non-randomized studies (901 patients) were identified. Meta-analysis showed that there was no significant difference between these two groups in 5-year overall survival rate [risk ratio (RR) 1.04 (95% CI: 0.93-1.16) for RCTs and 0.96 (95% CI: 0.83-1.10) for non-randomized studies] and post-operative mortality [RR 0.99 (95% CI: 0.44-2.24) for RCTs and 2.06 (95% CI: 0.69-6.15) for non-randomized studies]. There was a significant difference between these two groups in wound degree of surgery, operation time was significantly longer [weighted mean difference (WMD) 195.32 min (95% CI: 114.59-276.05) for RCTs and 126.07 min (95% CI: 22.09-230.04) for non-randomized studies] and blood loss was significantly greater [WMD 301 mL (95% CI: 151.55-450.45) for RCTs and 302.86 mL (95% CI: 127.89-477.84) for non-randomized studies] in D2 + PAND.
Conclusion: D2 + PAND can be performed as safely as standard D2 resection without increasing post-operative mortality but fail to benefit overall survival in patients with advanced gastric cancer.
Figures

References
-
- Parkin DM, Whelan SL, Ferlay J. Cancer Incidence in Five Continents, vol VII. Lyon, France: International Agency for Research on Cancer; 1997. pp. 822–823.
-
- Yamamoto S. Stomach cancer incidence in the world. Jpn J Clin Oncol. 2001;31:471. - PubMed
-
- Wang ZN, Lu C, Xu HM. Lymph node metastasis of upper gastric cancer and its significance in surgical treatment. Zhongguo Shiyong Waike Zazhi. 2002;22:611–612.
-
- Tsubono Y, Hisamichi S. Screening for gastric cancer in Japan. Gastric Cancer. 2000;3:9–18. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
