

A comparative epidemiologic analysis of SARS in Hong Kong, Beijing and Taiwan
- PMID: 20205928
- PMCID: PMC2846944
- DOI: 10.1186/1471-2334-10-50
A comparative epidemiologic analysis of SARS in Hong Kong, Beijing and Taiwan
Abstract
Background: The 2002-2003 Severe Acute Respiratory Syndrome (SARS) outbreak infected 8,422 individuals leading to 916 deaths around the world. However, there have been few epidemiological studies of SARS comparing epidemiologic features across regions. The aim of this study is to identify similarities and differences in SARS epidemiology in three populations with similar host and viral genotype.
Methods: We present a comparative epidemiologic analysis of SARS, based on an integrated dataset with 3,336 SARS patients from Hong Kong, Beijing and Taiwan, epidemiological and clinical characteristics such as incubation, onset-to-admission, onset-to-discharge and onset-to-death periods, case fatality ratios (CFRs) and presenting symptoms are described and compared between regions. We further explored the influence of demographic and clinical variables on the apparently large differences in CFRs between the three regions.
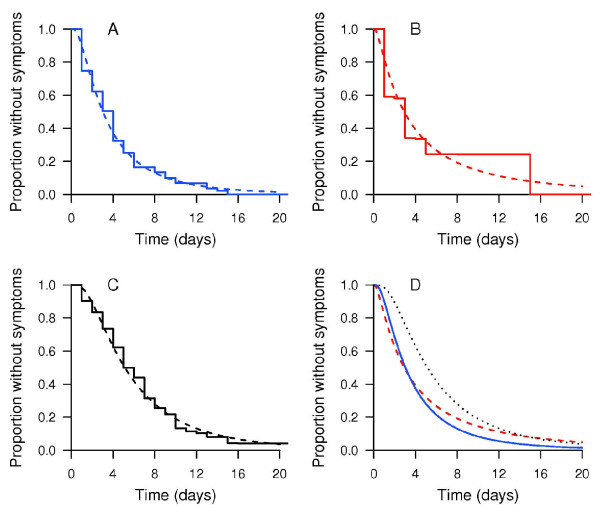
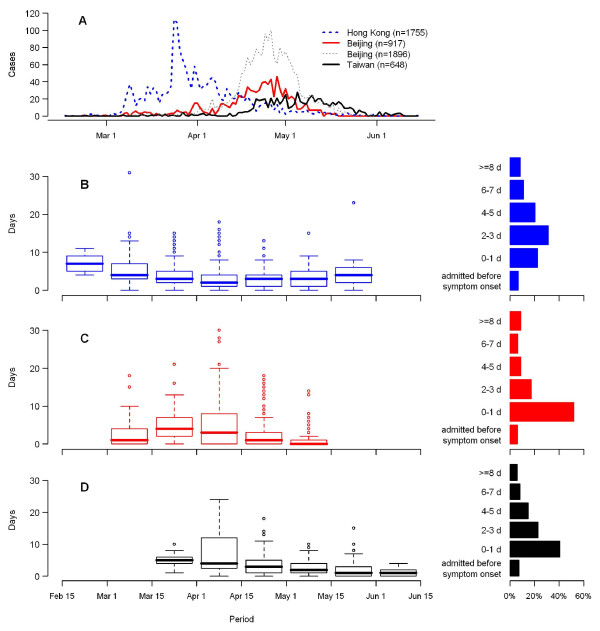
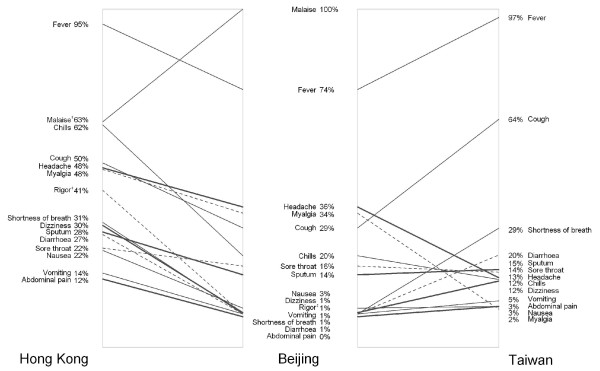
Results: All three regions showed similar incubation periods and progressive shortening of the onset-to-admission interval through the epidemic. Adjusted for sex, health care worker status and nosocomial setting, older age was associated with a higher fatality, with adjusted odds ratio (AOR): 2.10 (95% confidence interval: 1.45, 3.04) for those aged 51-60; AOR: 4.57 (95% confidence interval: 3.32, 7.30) for those aged above 60 compared to those aged 41-50 years. Presence of pre-existing comorbid conditions was also associated with greater mortality (AOR: 1.74; 95% confidence interval: 1.36, 2.21).
Conclusion: The large discrepancy in crude fatality ratios across the three regions can only be partly explained by epidemiological and clinical heterogeneities. Our findings underline the importance of a common data collection platform, especially in an emerging epidemic, in order to identify and explain consistencies and differences in the eventual clinical and public health outcomes of infectious disease outbreaks, which is becoming increasingly important in our highly interconnected world.
Figures
Similar articles
-
Investigation of a nosocomial outbreak of severe acute respiratory syndrome (SARS) in Toronto, Canada.CMAJ. 2003 Aug 19;169(4):285-92. CMAJ. 2003. PMID: 12925421 Free PMC article.
-
Epidemiological characteristics of an outbreak of severe acute respiratory syndrome in Dongcheng District of Beijing from March to May 2003.Biomed Environ Sci. 2003 Dec;16(4):305-13. Biomed Environ Sci. 2003. PMID: 15011961
-
The epidemiology of severe acute respiratory syndrome in the 2003 Hong Kong epidemic: an analysis of all 1755 patients.Ann Intern Med. 2004 Nov 2;141(9):662-73. doi: 10.7326/0003-4819-141-9-200411020-00006. Ann Intern Med. 2004. PMID: 15520422
-
[SARS: a new emergency in the world health].Recenti Prog Med. 2003 Jul-Aug;94(7-8):284-94. Recenti Prog Med. 2003. PMID: 12868233 Review. Italian.
-
Severe acute respiratory syndrome.Int J Tuberc Lung Dis. 2003 Dec;7(12):1117-30. Int J Tuberc Lung Dis. 2003. PMID: 14677886 Review.
Cited by
-
Investigating effects of healthcare simulation on personal strengths and organizational impacts for healthcare workers during COVID-19 pandemic: A cross-sectional study.Integr Med Res. 2020 Sep;9(3):100476. doi: 10.1016/j.imr.2020.100476. Epub 2020 Jul 16. Integr Med Res. 2020. PMID: 32802743 Free PMC article.
-
Assessment of transmissibility and measures effectiveness of SARS in 8 regions, China, 2002-2003.Front Cell Infect Microbiol. 2023 Aug 10;13:1212473. doi: 10.3389/fcimb.2023.1212473. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 37637464 Free PMC article.
-
On a Statistical Transmission Model in Analysis of the Early Phase of COVID-19 Outbreak.Stat Biosci. 2021;13(1):1-17. doi: 10.1007/s12561-020-09277-0. Epub 2020 Apr 2. Stat Biosci. 2021. PMID: 32292527 Free PMC article.
-
Estimation of incubation period distribution of COVID-19 using disease onset forward time: A novel cross-sectional and forward follow-up study.Sci Adv. 2020 Aug 14;6(33):eabc1202. doi: 10.1126/sciadv.abc1202. eCollection 2020 Aug. Sci Adv. 2020. PMID: 32851189 Free PMC article.
-
Pathogenesis of Middle East respiratory syndrome coronavirus.J Pathol. 2015 Jan;235(2):175-84. doi: 10.1002/path.4458. J Pathol. 2015. PMID: 25294366 Free PMC article. Review.
References
-
- Summary of probable SARS cases with onset of illness from 1 November 2002 to 7 August 2003. http://www.who.int/csr/sars/country/country2003_08_15.pdf
-
- CDC SARS Investigative Team. Update: outbreak of severe acute respiratory syndrome--worldwide, 2003. MMWR Morb Mortal Wkly Rep. 2003;52:269–272. - PubMed
-
- SARS outbreak contained worldwide. http://www.who.int/mediacentre/news/releases/2003/pr56/en/
-
- Escudero IH, Chen MI, Leo YS. Surveillance of severe acute respiratory syndrome (SARS) in the post-outbreak period. Singapore Med J. 2005;46:165–171. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
