

Identification of a recurrent microdeletion at 17q23.1q23.2 flanked by segmental duplications associated with heart defects and limb abnormalities
- PMID: 20206336
- PMCID: PMC2833380
- DOI: 10.1016/j.ajhg.2010.01.038
Identification of a recurrent microdeletion at 17q23.1q23.2 flanked by segmental duplications associated with heart defects and limb abnormalities
Abstract
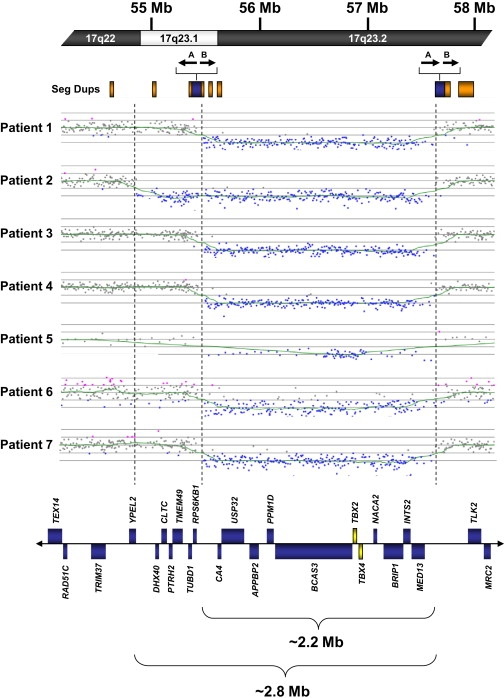
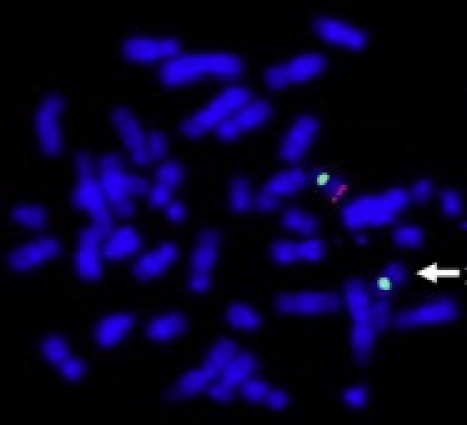
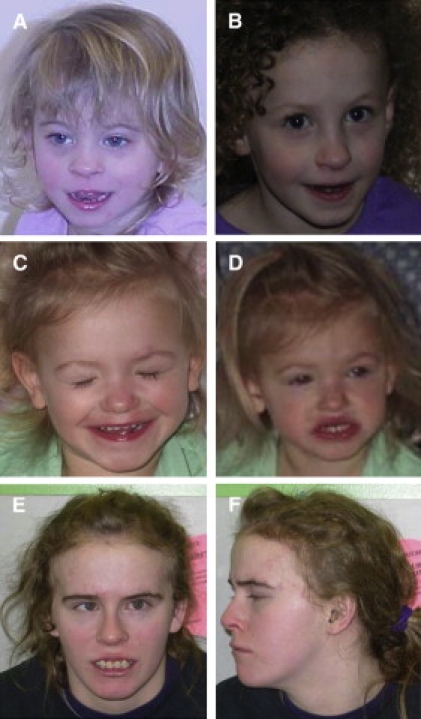
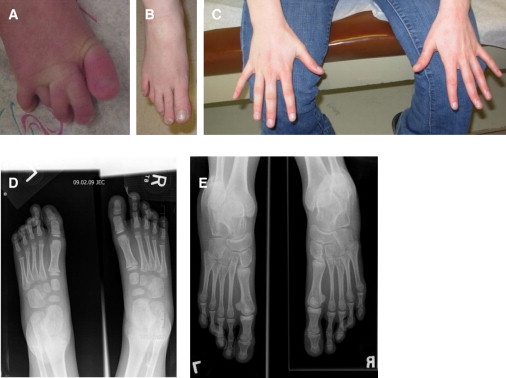
Segmental duplications, which comprise approximately 5%-10% of the human genome, are known to mediate medically relevant deletions, duplications, and inversions through nonallelic homologous recombination (NAHR) and have been suggested to be hot spots in chromosome evolution and human genomic instability. We report seven individuals with microdeletions at 17q23.1q23.2, identified by microarray-based comparative genomic hybridization (aCGH). Six of the seven deletions are approximately 2.2 Mb in size and flanked by large segmental duplications of >98% sequence identity and in the same orientation. One of the deletions is approximately 2.8 Mb in size and is flanked on the distal side by a segmental duplication, whereas the proximal breakpoint falls between segmental duplications. These characteristics suggest that NAHR mediated six out of seven of these rearrangements. These individuals have common features, including mild to moderate developmental delay (particularly speech delay), microcephaly, postnatal growth retardation, heart defects, and hand, foot, and limb abnormalities. Although all individuals had at least mild dysmorphic facial features, there was no characteristic constellation of features that would elicit clinical suspicion of a specific disorder. The identification of common clinical features suggests that microdeletions at 17q23.1q23.2 constitute a novel syndrome. Furthermore, the inclusion in the minimal deletion region of TBX2 and TBX4, transcription factors belonging to a family of genes implicated in a variety of developmental pathways including those of heart and limb, suggests that these genes may play an important role in the phenotype of this emerging syndrome.
Copyright 2010 The American Society of Human Genetics. Published by Elsevier Inc. All rights reserved.
Figures

Similar articles
-
Microdeletion of 17q22q23.2 encompassing TBX2 and TBX4 in a patient with congenital microcephaly, thyroid duct cyst, sensorineural hearing loss, and pulmonary hypertension.Am J Med Genet A. 2011 Feb;155A(2):418-23. doi: 10.1002/ajmg.a.33827. Epub 2011 Jan 13. Am J Med Genet A. 2011. PMID: 21271665
-
Identification of uncommon recurrent Potocki-Lupski syndrome-associated duplications and the distribution of rearrangement types and mechanisms in PTLS.Am J Hum Genet. 2010 Mar 12;86(3):462-70. doi: 10.1016/j.ajhg.2010.02.001. Epub 2010 Feb 25. Am J Hum Genet. 2010. PMID: 20188345 Free PMC article.
-
Two new cases with microdeletion of 17q23.2 suggest presence of a candidate gene for sensorineural hearing loss within this region.Am J Med Genet A. 2011 Dec;155A(12):2964-9. doi: 10.1002/ajmg.a.34302. Epub 2011 Nov 3. Am J Med Genet A. 2011. PMID: 22052739
-
Molecular characterization of a patient with 3p deletion syndrome and a review of the literature.Am J Med Genet A. 2008 Nov 1;146A(21):2746-52. doi: 10.1002/ajmg.a.32533. Am J Med Genet A. 2008. PMID: 18837054 Review.
-
The discovery of microdeletion syndromes in the post-genomic era: review of the methodology and characterization of a new 1q41q42 microdeletion syndrome.Genet Med. 2007 Sep;9(9):607-16. doi: 10.1097/gim.0b013e3181484b49. Genet Med. 2007. PMID: 17873649 Review.
Cited by
-
Genetics and Other Omics in Pediatric Pulmonary Arterial Hypertension.Chest. 2020 May;157(5):1287-1295. doi: 10.1016/j.chest.2020.01.013. Epub 2020 Jan 30. Chest. 2020. PMID: 32006592 Free PMC article. Review.
-
First Genotype-Phenotype Study in TBX4 Syndrome: Gain-of-Function Mutations Causative for Lung Disease.Am J Respir Crit Care Med. 2022 Dec 15;206(12):1522-1533. doi: 10.1164/rccm.202203-0485OC. Am J Respir Crit Care Med. 2022. PMID: 35852389 Free PMC article.
-
Genes in pediatric pulmonary arterial hypertension and the most promising BMPR2 gene therapy.Front Genet. 2022 Nov 24;13:961848. doi: 10.3389/fgene.2022.961848. eCollection 2022. Front Genet. 2022. PMID: 36506323 Free PMC article. Review.
-
Complex Phenotypes: Mechanisms Underlying Variation in Human Stature.Curr Osteoporos Rep. 2019 Oct;17(5):301-323. doi: 10.1007/s11914-019-00527-9. Curr Osteoporos Rep. 2019. PMID: 31441021 Free PMC article. Review.
-
Tbx2a is required for specification of endodermal pouches during development of the pharyngeal arches.PLoS One. 2013 Oct 10;8(10):e77171. doi: 10.1371/journal.pone.0077171. eCollection 2013. PLoS One. 2013. PMID: 24130849 Free PMC article.
References
-
- Bailey J.A., Gu Z., Clark R.A., Reinert K., Samonte R.V., Schwartz S., Adams M.D., Myers E.W., Li P.W., Eichler E.E. Recent segmental duplications in the human genome. Science. 2002;297:1003–1007. - PubMed
-
- Shaffer L.G., Lupski J.R. Molecular mechanisms for constitutional chromosomal rearrangements in humans. Annu. Rev. Genet. 2000;34:297–329. - PubMed
-
- Stankiewicz P., Lupski J.R. Genome architecture, rearrangements and genomic disorders. Trends Genet. 2002;18:74–82. - PubMed
-
- Koolen D.A., Vissers L.E., Pfundt R., de Leeuw N., Knight S.J., Regan R., Kooy R.F., Reyniers E., Romano C., Fichera M. A new chromosome 17q21.31 microdeletion syndrome associated with a common inversion polymorphism. Nat. Genet. 2006;38:999–1001. - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
- Actions
- Actions
- Actions
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
