

Ex vivo imaging of human thyroid pathology using integrated optical coherence tomography and optical coherence microscopy
- PMID: 20210448
- PMCID: PMC2844129
- DOI: 10.1117/1.3306696
Ex vivo imaging of human thyroid pathology using integrated optical coherence tomography and optical coherence microscopy
Abstract
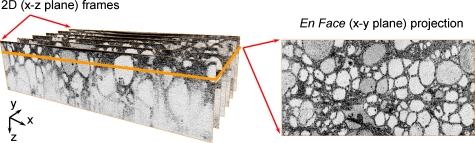
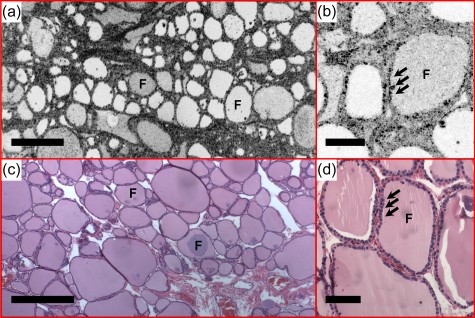
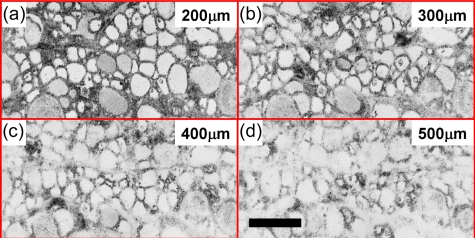
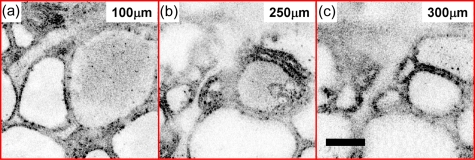
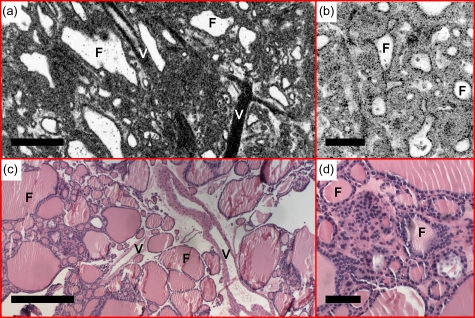
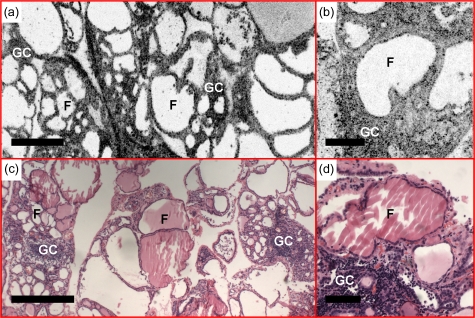
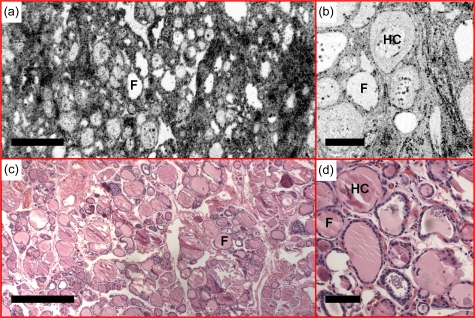
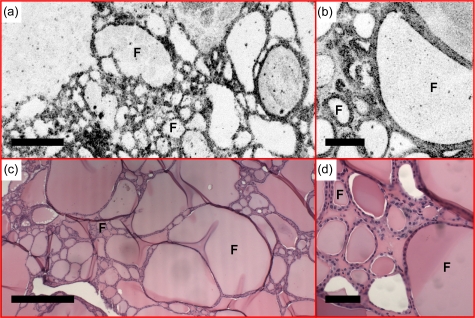
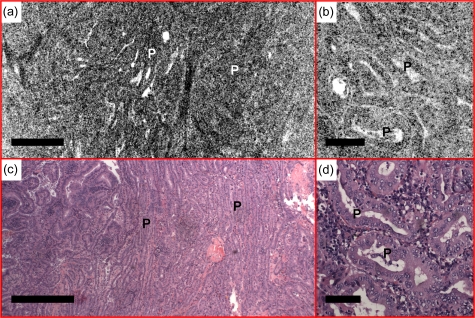
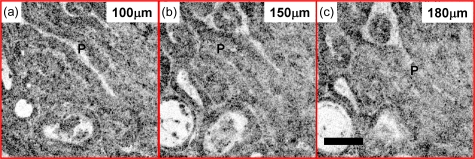
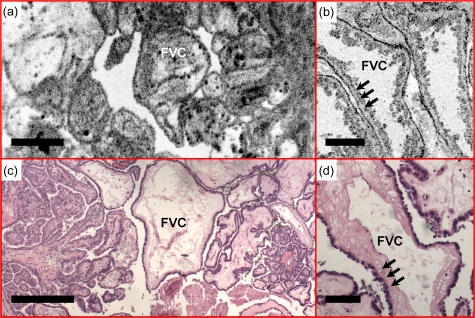
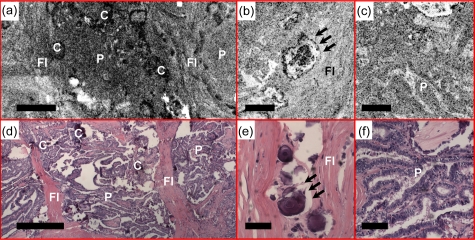
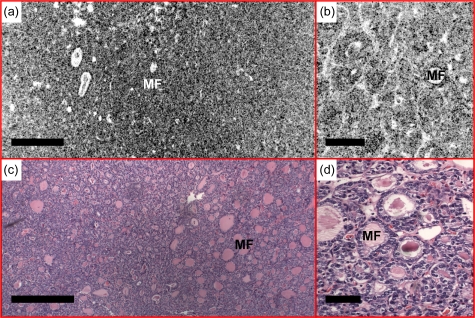
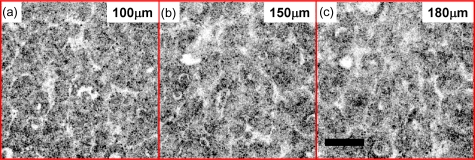
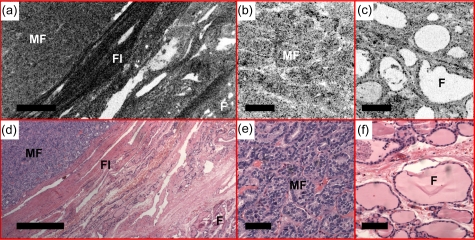
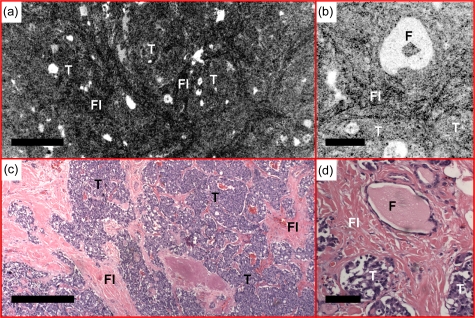
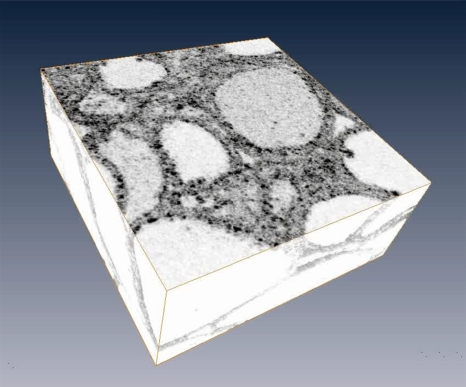
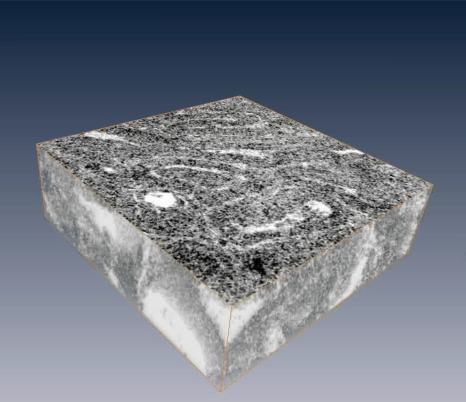
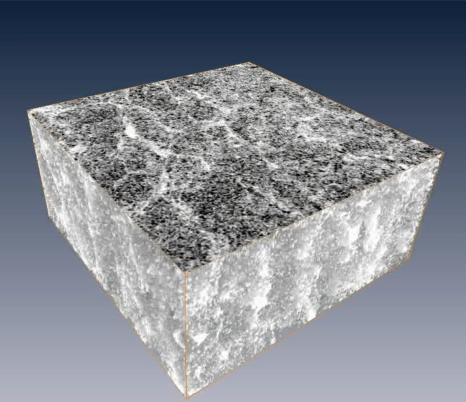
We evaluate the feasibility of optical coherence tomography (OCT) and optical coherence microscopy (OCM) for imaging of benign and malignant thyroid lesions ex vivo using intrinsic optical contrast. 34 thyroid gland specimens are imaged from 17 patients, covering a spectrum of pathology ranging from normal thyroid to benign disease/neoplasms (multinodular colloid goiter, Hashimoto's thyroiditis, and follicular adenoma) and malignant thyroid tumors (papillary carcinoma and medullary carcinoma). Imaging is performed using an integrated OCT and OCM system, with <4 microm axial resolution (OCT and OCM), and 14 microm (OCT) and <2 microm (OCM) transverse resolution. The system allows seamless switching between low and high magnifications in a way similar to traditional microscopy. Good correspondence is observed between optical images and histological sections. Characteristic features that suggest malignant lesions, such as complex papillary architecture, microfollicules, psammomatous calcifications, or replacement of normal follicular architecture with sheets/nests of tumor cells, can be identified from OCT and OCM images and are clearly differentiable from normal or benign thyroid tissues. With further development of needle-based imaging probes, OCT and OCM could be promising techniques to use for the screening of thyroid nodules and to improve the diagnostic specificity of fine needle aspiration evaluation.
Figures
References
-
- Cancer Facts and Figures, American Cancer Society, Atlanta, GA: (2009).
-
- Wiest P. W., Hartshorne M. F., Inskip P. D., Crooks L. A., Vela B. S., Telepak R. J., Williamson M. R., Blumhardt R., Bauman J. M., and Tekkel M., “Thyroid palpation versus high-resolution thyroid ultrasonography in the detection of nodules,” J. Ultrasound Med. 17, 487–496 (1998). - PubMed
-
- Carroll B. A., “Asymptomatic thyroid-nodules—incidental sonographic detection,” Am. J. Roentgenol. 138, 499–501 (1982). - PubMed
-
- Brander A., Viikinkoski P., Nickels J., and Kivisaari L., “Thyroid-gland—ultrasound screening in a random adult-population,” Radiology 181, 683–687 (1991). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
