

Diagnosis and follow-up of treatment of latent tuberculosis; the utility of the QuantiFERON-TB Gold In-tube assay in outpatients from a tuberculosis low-endemic country
- PMID: 20210999
- PMCID: PMC2842274
- DOI: 10.1186/1471-2334-10-57
Diagnosis and follow-up of treatment of latent tuberculosis; the utility of the QuantiFERON-TB Gold In-tube assay in outpatients from a tuberculosis low-endemic country
Abstract
Background: Interferon-gamma (IFN-gamma) Release Assays (IGRA) are more specific than the tuberculosis skin test (TST) in the diagnosis of latent tuberculosis (TB) infection (LTBI). We present the performance of the QuantiFERON-TB Gold In-tube (QFT-TB) assay as diagnostic test and during follow-up of preventive TB therapy in outpatients from a TB low-endemic country.
Methods: 481 persons with suspected TB infection were tested with QFT-TB. Thoracic X-ray and sputum samples were performed and a questionnaire concerning risk factors for TB was filled. Three months of isoniazid and rifampicin were given to patients with LTBI and QFT-TB tests were performed after three and 15 months.
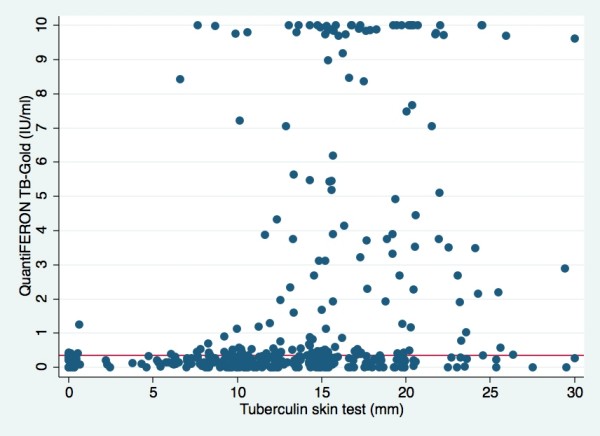
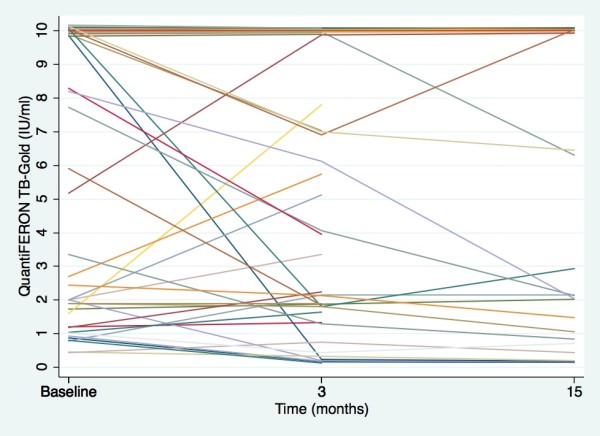
Results: The QFT-TB test was positive in 30.8% (148/481) of the total, in 66.9% (111/166) of persons with origin from a TB endemic country, in 71.4% (20/28) previously treated for TB and in 100% (15/15) of those diagnosed with active TB with no inconclusive results. The QFT-TB test was more frequently positive in those with TST > or = 15 mm (47.5%) compared to TST 11-14 mm (21.3%) and TST 6-10 mm (10.5%), (p < 0.001). Origin from a TB endemic country (OR 6.82, 95% CI 1.73-26.82), recent stay in a TB endemic country (OR 1.32, 95% CI 1.09-1.59), duration of TB exposure (OR 1.59, 95% CI 1.14-2.22) and previous TB disease (OR 11.60, 95% CI 2.02-66.73) were all independently associated with a positive QFT-TB test. After preventive therapy, 35/40 (87.5%) and 22/26 (84.6%) were still QFT-TB positive after three and 15 months, respectively. IFN-gamma responses were comparable at start (mean 6.13 IU/ml +/- SD 3.99) and after three months (mean 5.65 IU/ml +/- SD 3.66) and 15 months (mean 5.65 IU/ml +/- SD 4.14), (p > 0.05).
Conclusion: Only one third of those with suspected TB infection had a positive QFT-TB test. Recent immigration from TB endemic countries and long duration of exposure are risk factors for a positive QFT-TB test and these groups should be targeted through screening. Since most patients remained QFT-TB positive after therapy, the test should not be used to monitor the effect of preventive therapy. Prospective studies are needed in order to determine the usefulness of IGRA tests during therapy.
Figures
Similar articles
-
[The clinical application of quantiferon TB-2G: its usefulness and limitations].Kekkaku. 2011 Feb;86(2):101-12. Kekkaku. 2011. PMID: 21404654 Japanese.
-
QuantiFERON-TB Gold In-Tube Test for Tuberculosis Prevention in HIV-Infected Patients.Jpn J Infect Dis. 2017 Sep 25;70(5):502-506. doi: 10.7883/yoken.JJID.2016.480. Epub 2017 Mar 28. Jpn J Infect Dis. 2017. PMID: 28367883
-
Screening for latent tuberculosis in Norwegian health care workers: high frequency of discordant tuberculin skin test positive and interferon-gamma release assay negative results.BMC Public Health. 2013 Apr 17;13:353. doi: 10.1186/1471-2458-13-353. BMC Public Health. 2013. PMID: 23590619 Free PMC article.
-
[Evolution of IGRA researches].Kekkaku. 2008 Sep;83(9):641-52. Kekkaku. 2008. PMID: 18979999 Review. Japanese.
-
Interferon-γ release assays or tuberculin skin test for detection and management of latent tuberculosis infection: a systematic review and meta-analysis.Lancet Infect Dis. 2020 Dec;20(12):1457-1469. doi: 10.1016/S1473-3099(20)30276-0. Epub 2020 Jul 13. Lancet Infect Dis. 2020. PMID: 32673595
Cited by
-
Long-term follow-up after treatment of tubercular uveitis: case series and review of the literature.Front Ophthalmol (Lausanne). 2023 Nov 17;3:1270948. doi: 10.3389/fopht.2023.1270948. eCollection 2023. Front Ophthalmol (Lausanne). 2023. PMID: 38983011 Free PMC article.
-
Inflammatory markers and clinical characteristics for predicting persistent positivity of interferon gamma release assay in dialysis population.Sci Rep. 2016 Oct 5;6:34577. doi: 10.1038/srep34577. Sci Rep. 2016. PMID: 27703202 Free PMC article. Clinical Trial.
-
Challenges in Developing a Controlled Human Tuberculosis Challenge Model.Curr Top Microbiol Immunol. 2024;445:229-255. doi: 10.1007/82_2022_252. Curr Top Microbiol Immunol. 2024. PMID: 35332386 Review.
-
CD4 response of QuantiFERON-TB Gold Plus for positive consistency of latent tuberculosis infection in patients on dialysis.Sci Rep. 2020 Dec 7;10(1):21367. doi: 10.1038/s41598-020-78374-3. Sci Rep. 2020. PMID: 33288814 Free PMC article.
-
Risk of Tuberculosis Among Patients on Dialysis: The Predictive Value of Serial Interferon-Gamma Release Assay.Medicine (Baltimore). 2016 May;95(22):e3813. doi: 10.1097/MD.0000000000003813. Medicine (Baltimore). 2016. PMID: 27258523 Free PMC article.
References
-
- Lalvani A, Pathan AA, McShane H. Rapid detection of Mycobacterium tuberculosis infection by enumeration of antigen-specific T cells. Am J Respir Crit Care Med. 2001;163:824–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
